
Abstract
The study compares the association between using the services of commercial sex workers and male HIV seroprevalence in five African countries: Ghana, Kenya, Lesotho, Malawi and Rwanda. The HIV seroprevalence among men who ‘ever paid for sex’ was compared with controls who ‘never paid for sex’. Results were based on 12,929 eligible men, aged 15–59 years, interviewed in Demographic and Health Surveys. The odds ratio of HIV seroprevalence associated with ever paying for sex was 1.89 (95% confidence interval = 1.57–2.28), with only minor differences by country. The results were stable in multivariate analysis after controlling for available potential cofactors (data on non-sexual routes of transmission were not available). Given the relatively small proportion of men involved, the risk attributable to ‘ever paying for sex’ remained low: 7.1% in univariate analysis and 4.4% after adjustment, and it varied among countries (range 1.3–9.4%). These results match previous observations that commercial sex seems to play a minor role in the spread of HIV in mature epidemics.
Keywords
Introduction
The fast onset of the HIV epidemic in the mid-1980s in sub-Saharan Africa surprised many investigators. From the earlier studies, the role of commercial sex was considered the main source of spreading the disease in heterosexual epidemics.1–3 Many female commercial sex workers (CSWs) became quickly infected, with HIV seroprevalence rates of 50% and above in large cities such as Kinshasa (Zaire), Nairobi (Kenya) or Abidjan (Cote d'Ivoire) within a few years after onset of the epidemics.4–11 Many of their male partners were also infected and the number of partners was found to be at a critical risk factor for HIV infection. This led to a major imbalance between the two genders, with larger numbers of men infected and dying of AIDS than women. Similar findings were found a few years later in Asia, in particular in Thailand and India, where heterosexual transmission was deemed to be important among CSWs and their clients.12–17
If the rationale of the spread of the disease became soon well understood in the early years of the epidemics, the situation is quite different some 20 years later, when HIV transmission became a feature of the general population, without any obvious universal risk factor and with a balance between genders or an excess of women over men infected with HIV.18–20
This new situation questions the role of commercial sex in the spread of HIV in mature epidemics. This issue is rather complex, since the HIV prevalence among CSWs varies by country, the practice of commercial sex by women varies greatly among countries, and is also very diverse within the same country.3,20–25 The use of CSWs services by men also varies by country and according to a variety of factors within the same country, such as age, marital status, urbanization, education, migration, poverty, ethnicity, religion and probably many other factors.14,26–30 The consequences are also different for men and women, since many more men are involved than women, and since this behaviour implies higher number of partners for women, and therefore higher risk of contracting HIV.22,31–33
HIV seroprevalence among female CSWs is rather well documented in Africa, and an international database was built by the USA Bureau of the Census,18,19 later taken over by UNAIDS. 20 The results show high rates of infection, among CSWs, with mean around 40% and a range from 30% to 90%, with some exceptions with much lower values, such as Chad, Equatorial Guinea, Madagascar, Seychelles Islands and Senegal. In contrast, much less is known on the male clients of CSWs. A study conducted in a rural community in Zimbabwe found an attributable risk of HIV infection due to visiting CSWs equal to 19.6% (95% confidence interval [CI] = [10.8–27.6]). 28 In contrast, the four-city study conducted in two cities of high prevalence (Kisumu, Kenya and Ndola, Zambia) and two cities of low prevalence (Cotonou, Benin and Yaoundé, Cameroon) concluded that sex work did not explain the differential spread of the HIV epidemic among countries. 22 Using broad international comparisons and vague estimates of the number of female CSWs, Talbott 34 found a correlation between the number of CSWs and HIV prevalence levels across African countries. The role of commercial sex on male HIV infection remains therefore controversial, and the situations may differ from country to country.
This study aims at shedding some light on this debate by approaching the problem from a demographic perspective. The demographic and health surveys (DHS) allow one to compare the HIV seroprevalence among clients and non-clients of CSWs, and also to determine the proportion of men who ever used these services. These two types of information (prevalence and relative risk) allow one to compute the attributable risk of contracting HIV associated with using the services of CSWs. The data that were used were collected in the early 2000s, and all countries investigated could be classified as situations of ‘mature epidemics’.
Material and Methods
Study population
Data used for this analysis come from the DHS, which are surveys conducted on nationally representative samples of men and women in their reproductive ages. 35 They provide data on numerous demographic and health characteristics, as well as on sexual behaviour. Various elements of sexual behaviour are available in DHS surveys, and in some of them a question was asked to men aged 15–59 whether they ‘ever paid for sex’. Furthermore, since 2001, some of the recent studies include data on HIV seroprevalence.
In sub-Saharan Africa, 12 DHS surveys with information on HIV were available at the time of this study, five of which permitted the matching of the HIV serological status with that on ‘ever paid for sex’: Ghana 2003, Kenya 2003, Lesotho 2004, Malawi 2004 and Rwanda 2005.
The study population is therefore composed of men aged 15–59 years, who ever had sex, who answered the question ‘Have you ever paid for sex?’, and with a known HIV serological status. Men who had answered ‘yes’ to the question ‘Ever paid for sex?’ will be called ‘CSWs clients’ in this paper.
Data analysis
The five DHS surveys were first analysed separately, and then pooled together for the combined analysis. In the univariate analysis, the HIV status of men who had ever visited CSWs was compared with that of men reporting no visit at the time of survey. In the multivariate analysis, the odds ratios (OR) of HIV prevalence were estimated by a linear logistic regression model, which included, in addition to visiting CSWs, several adjustment variables: age (linear, in years), marital status (never married, married or formerly married), time since first intercourse (linear, in years), place of residence (rural versus urban), level of education (low, medium or high) and number of sexual partners in the last 12 months (0, 1 or 2 and more). Age and time since first intercourse were measures of duration of exposure to HIV infection by sexual contacts. Marital status and number of partners in the last 12 months were other factors of sexual activity. Finally, level of education and the place of residence could be potential confounders of HIV prevalence and of sexual behaviour. In the pooled analysis, we added the country as an adjustment variable, since prevalence differed widely from country to country. The statistical analysis was conducted with Stata 9.0 statistical software (Stata Corp., College Station, TX, USA).
Results
Basic data
Of the 24,120 men aged 15–59 years interviewed in the five DHS surveys, 12,929 men (53.6%) were eligible for this study, as being sexually active, having answered the question ‘Have you ever paid for sex?’ and having a known HIV serological status. The HIV prevalence differed between countries and ranged from 2.0% in Ghana, 3.3% in Rwanda, 5.1% in Kenya, 11.1% in Malawi and 21.8% in Lesotho (Table 1). The proportions of men who ever paid for sex also differed among the countries and ranged from 1.1% in Rwanda, 6.4% in Lesotho, 8.1% in Ghana, 15.3% in Kenya and 21.8% in Malawi (Table 1). Overall, the correlation among countries between HIV seroprevalence and proportions who ever paid for sex was negative and not significant (Pearson correlation coefficient = –0.626; 95% CI = [–0.972; 0.572]; P = 0.26).
Sample size and basic data on HIV seroprevalence and the use of commercial sex
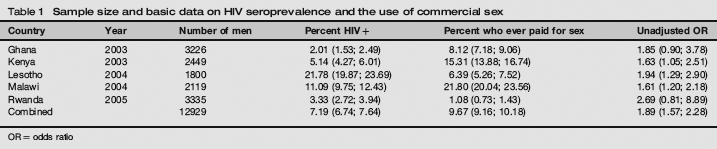
OR = odds ratio
At the individual level, in univariate analysis, CSWs clients had consistently higher HIV seroprevalence in the five countries investigated, and significantly so in Kenya (OR = 1.63; P = 0.028), Lesotho (OR = 1.94; P = 0.001) and Malawi (OR = 1.61; P = 0.002) (Table 1). The combined OR was highly significant in the merged dataset (OR = 1.89; 95% CI = [1.57–2.28], P < 0.001). Note that all the OR investigated were of the same magnitude in the five countries (range: 1.61–2.69), a good indication of consistency across countries.
Factors of HIV Prevalence
Available potential confounding factors of the association between using CSWs services and HIV seroprevalence are detailed in Table 2, which summarizes the raw effect of each variable in the pooled sample. All differences investigated were significant: there was a large country effect, already noted above (P < 0.001); age was positively associated with HIV (P < 0.001); marital status was also associated with HIV, with higher prevalence for married and formerly married men (P < 0.001); urban areas had higher prevalence than rural areas (P < 0.011); the number of partners in the last 12 months was significant (P < 0.001); surprisingly when compared with previous publications, increasing level of education was associated with reduced risk of HIV (P = 0.036) and time since first intercourse had an effect similar to that of age (P < 0.001).
Univariate analysis of the risk factors of HIV seroprevalence, pooled sample
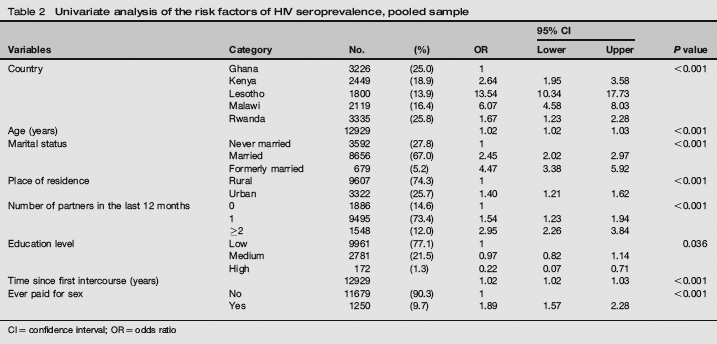
CI = confidence interval; OR = odds ratio
These variables were used as controls for running the multivariate analysis, with the exception of age that was too heavily correlated with time since first intercourse, and dropped in the final model (Table 3). In the multivariate analysis of the merged dataset, the OR of HIV prevalence remained strongly associated with ‘ever paid for sex’, with an adjusted value similar to the raw effect (OR = 1.50, 95% CI = 1.21–1.84, P < 0.001), which confirms the order of magnitude of the association, and indicates an absence of major confounders within available potential cofactors. Furthermore, the effects of the covariates remained by and large similar to those found in the univariate analysis. The hierarchy of countries remained similar, which means that the intercountry differences could not be explained by the covariates investigated. The effect of marital status remained similar; the effect of urban residence was somewhat increased (1.96 instead of 1.40), the effect of number of partners in last 12 months was reduced (1.17 instead of 2.95); however, the effect of a medium level of education became higher than one, and the effect of higher education became no longer significant; the effect of time since first intercourse kept a similar value.
Multivariate analysis of the risk factors of HIV seroprevalence, pooled dataset

CI = confidence interval; OR = odds ratio
We ran the same type of model in each country separately. Overall, the effect of payment for sex remained consistent. CSWs clients had a higher risk of HIV infection than non-clients, significantly so in Lesotho (OR = 1.54; P = 0.049) and in Malawi (OR = 1.59; P = 0.004) (Table 4). In summary, the significantly higher risk of HIV infection associated with using commercial sex services found in univariate analysis was confirmed in the multivariate analysis.
Estimates of the risk of HIV seroprevalence attributable to use of commercial sex, men age 15–54
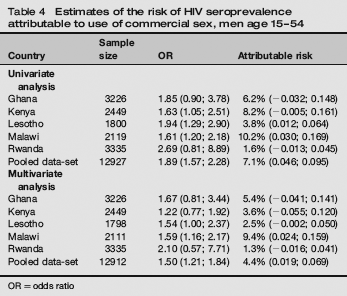
OR = odds ratio
Attributable risk
Knowing the OR and the prevalence of ‘payment for sex’ allows one to estimate the attributable fraction, that is the proportion of HIV prevalence explained by this behaviour. Overall, the HIV risk attributable to ‘ever paid for sex’ was only 7.1% in univariate analysis and 4.4% after adjustment for the five countries combined (Table 4). Of course, this attributable risk varied by country, not because of the relative risks, which were homogeneous among countries, but because of the varying proportions of men who ever paid for sex. The estimated adjusted attributable risk varied for 1.3% in Rwanda, 2.5% in Lesotho, 3.6% in Kenya, 5.4% in Ghana and 9.4% in Malawi. Note again that there was no evident correlation between the attributable fraction and the level of HIV prevalence in the country, one more indication that other factors explained the differences in HIV prevalence.
Discussion
Our estimate of a small fraction of men's HIV infections attributable to ‘ever paid for sex’, seems to indicate that commercial sex played a relatively small role in the spread of HIV in mature epidemics, whatever the level of infection in the population. This finding matches that of the four-city study, which also found a small effect of commercial sex in four African cities located in different countries, and with different levels of HIV infection. 22
The consistency of the OR between countries and the absence of any major confounder, within the available tested cofactors, indicates that the risk associated with being a client of CSWs is a feature of mature epidemics, that is a spread of the virus into the general population beyond core groups or high-risk groups, within two or three decades after onset. This property seems to be largely independent from the level of seroprevalence of the epidemic.
Of course, this does not imply that commercial sex did not play a role in the first phase of the epidemic. Numerous examples throughout Africa are here to remind us that a large proportion of the first HIV/AIDS cases occurred among female CSWs and their clients, whether in Abidjan (Cote d'Ivoire), in Dakar (Senegal), in Nairobi (Kenya), in Mombasa (Kenya) and in large cities of South Africa.5,9,36,37 Many studies have confirmed the high rate of infection among female CSWs, often higher than 50%, and even reaching 80% or more. 23 Commercial sex obviously played a major role in spreading the disease in the general population in the early years. However, this does not imply that most men's infections now come from this source. With a 7.2% of men infected on average, and a 4.4% attributable risk, some 0.3% of the male population seems to have been infected through commercial sex, a proportion still below the 1% threshold considered as necessary for an increase towards a generalized epidemic.
Other authors tried to explain differences in HIV seroprevalence by the extent of commercial sex in each country. 34 Our study does not confirm this assertion. On the contrary, the country the most heavily infected (Lesotho) had one of the smallest proportion of men using commercial sex services and one of the lowest attributable risk, and likewise in Kenya HIV prevalence was below average, whereas the proportion of CSW's clients was above average.
One could also question the validity of the answers to such a sensitive question ‘have you ever paid for sex?’. However, the proportions found seem reasonable and certainly consistent with other surveys conducted elsewhere. Furthermore, the proportion of men who ever paid for sex seems to be compatible with the work of the female CSWs. Another indication of validity of the DHS questions is the consistency of the effect between countries.
Differences in the proportions of men who ever paid for sex among countries, the critical determinant of attributable risks, may be due to a variety of social and behavioural factors. First, an overview of the many studies conducted in Africa reveals the great variety of forms of prostitution throughout Africa, from women who have only a few clients a week, to women who have several clients a night.11,31,38 For instance, Nagot et al. 32 in Burkina-Faso distinguished six main categories of CSWs (two professional and four non-professional) with different sexual behaviours. Their mean numbers of clients ranged from 2.1 per week for non-professional ‘students’ to 28.3 per week for professional ‘seaters’ and of course, these had different levels of HIV prevalence. Secondly, the geographical spread of prostitution seems to be also highly variable, from being located primarily in a single spot (a harbour or an industrial centre in some countries) or being widely available in most urban centres. Thirdly, the use of CSWs services by men may also depend on a variety of factors, both economical and social or religious, some societies being more permissive than others, which engenders large discrepancies between regions. 27 Lastly, migration and travels are also major vectors of HIV transmission, and this includes also moves from CSWs themselves. Within countries, female sex workers are often concentrated along the side of main roads where truck drivers are their main clients.
This study focused on heterosexual transmission of HIV, for which data were available in DHS surveys. Of course, other modes of HIV transmission could be considered as well, such as intravenous drug use or other exposures to infected blood through traditional or medical procedures. 39 However, we could not figure out a typical confounder that could explain the pattern found in this study, and in particular the consistency in OR across countries. Of course, only more information on all types of exposure to HIV could help sorting out this thorny issue.
Condom use remained limited in Africa in the early years of the HIV epidemics, even among CSWs and their clients.29,40 However, this has been changing quickly in the recent years, and this new behaviour could have changed the magnitude of the effect of commercial sex on HIV spread. 41 In Abidjan, Côte d'Ivoire, HIV prevalence fell from 89% in 1992 to 32% in 1998 among sex workers attending an STI clinic (Clinique de Confiance) for the first time, mainly because of an increase of condom use (P < 0.001). 42
Even though our analysis shows that the attributable risk associated with ever paying for sex is now small, whatever could be gained by reducing transmission between CSWs and their clients would benefit to the whole population in the long term.