
Abstract
Summary:
The availability of antiretroviral therapy has dramatically reduced the risk of HIV mother-to-child transmission (MTCT). However, mothers infected with multidrug resistant HIV (MDR-HIV) are at increased risk of MTCT. We report the case of a pregnant patient infected with MDR-HIV in whom MTCT was avoided with enfuvirtide use in late pregnancy and elective caesarean section.
Introduction
The use of antiretroviral therapy (ART) has reduced the risk of mother-to-child transmission (MTCT) of HIV to less than 2% in Europe. 1 With the improvement of clinical conditions following the introduction of highly active ART (HAART), the number of HIV-infected females who remain pregnant, even if infected with multidrug resistant HIV (MDR-HIV), is increasing. Clinical trials demonstrated enfuvirtide potency against MDR-HIV2,3 but data regarding its safety during pregnancy and efficacy in preventing MTCT are scarce.
Case Report
We report the case of a 34-year-old female with an HIV infection in CDC stage B3 diagnosed in 1994. She has never been fully adherent to antiretroviral therapy which she started in 1995 with mono and dual nucleoside reverse transcriptase inhibitors (NRTI). She initiated HAART in 1998 with stavudine, lamivudine and indinavir, later simplified to stavudine, didanosine and nevirapine in June 1999. Nevirapine was discontinued shortly after because of allergy and replaced with nelfinavir. In September 2002, after a virological failure, she started a new regimen with saquinavir, didanosine and stavudine, the latter replaced later with lamivudine because of lipoatrophy. On April 2005, she referred she was at nine-week gestation and that she had suspended all antiretrovirals three months before. At that moment her HIV-RNA was 28,000 copies/mL and her CD4 count 497×106 cells/L. She was prescribed lamivudine, didanosine and saquinavir/ritonavir. One and two months later, her HIV-RNA was 530 and 580 copies/mL, respectively, and CD4 count remained stable. Four weeks later, her CD4 count was 683×106 cells/L and HIV-RNA was 13,000 copies/mL. A genotypic resistance test evidenced M41L, V118L, M184V and T215Y mutations in the reverse transcriptase and D30N, F53L, I54V, L63P, A71V, N88D and L90M in the protease. Her regimen was changed to lamivudine, didanosine and atazanavir/ritonavir with a reduction of HIV-RNA (4100 copies/mL) and a raise in CD4 count one-month later when she was in 34 weeks of gestation. Enfuvirtide was then added to her therapy. Two weeks later, her HIV-RNA was undetectable and her CD4 count was 845 × 106 cells/L. Enfuvirtide was well tolerated with only mild injection site reactions. In her 38th week of gestation, she underwent an elective caesarean section before and during which she received zidovudine according to PACTG 076. 4 She gave birth to an apparently healthy female newborn weighing 3.1 kg. The baby received lamivudine, zidovudine and nevirapine as prophylaxis. Its HIV-RNA was undetectable at birth, day 7, and months 1, 3, 6 and 12 after delivery. The mother's immunovirological response to HAART according to the week of gestation is shown in Figure 1.
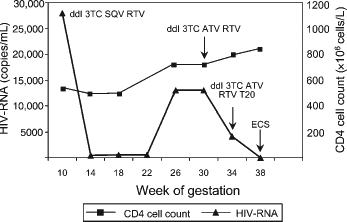
Virological and immunological response to HAART during pregnancy in a multidrug experienced HIV-infected patient. ddl: didanosine; 3TC: lamivudine; SQV: saquinavir; RTV: ritonavir; ATV: atazanavir; T20: enfuvirtide; ECS: elective cesarean section
Discussion
The risk of MTCT of HIV increases with gestational age as it has been estimated that fewer than 2% of infants acquire the infection more than two months before birth, while nearly 35% within two months before birth. In the remaining 65% of cases, MTCT occurs at birth via direct contact of the infant with infectious maternal blood and genital secretions during passage through the birth canal.5,6
Only a few cases of enfuvirtide use in late pregnancy to prevent MTCT of MDR-HIV are reported in literature. 7 10
In four of five cases the mothers’ plasma HIV-RNA ranged from less than 50 to 305 copies/mL at labour and these patients underwent an elective caesarean section avoiding transmission to the infant. In the remaining case, even though the mother's plasma HIV-RNA was undetectable, her baby became infected with MDR-HIV during the vaginal delivery. 8
Since enfuvirtide cannot cross the placenta, we hypothesize that, in our patient, HIV-RNA suppression reduced the probability for HIV to cross the placenta barrier. 9
Plasma and genital HIV-RNA are related in HIV-infected women and therefore, a reduction in both compartments occurs in most patients after HAART initiation. However, a response in plasma is associated with a failure to suppress HIV-RNA in the genital tract in some patients. 11
Thus, since enfuvirtide, the only fully active drug, cannot penetrate both the male and female genital tract, a dissociation between blood and genital tract HIV-RNA was possible in our patient.9,12 Elective caesarean section reduced the risk of HIV transmission at birth and should be, in our opinion, the preferred delivery mode in MDR-HIV-infected females, who should be considered at risk for MTCT even though if plasma HIV-RNA is undetectable.
In conclusion, although no definitive conclusions can be drawn by a single case report, we suggest that enfuvirtide use in the last month of gestation could represent a strategy to suppress plasma viral load and avoid in utero transmission of MDR-HIV.