
Abstract
Summary:
The aim of the present study was to evaluate the use of various serological tests in the diagnosis of early syphilis. The Murex enzyme immunoassay (EIA) test was used for screening; the Venereal Diseases Research Laboratory (VDRL) test, the Treponema pallidum particle agglutination assay (TPPA) and the Mercia antitreponemal IgM EIA were used in all the patients with a positive screening test and in those with suspected syphilis or in known contacts. In 89 cases of primary syphilis, the Murex EIA screening test was positive in 67 (75%) patients, the Mercia IgM EIA in 80 (90%) cases, the VDRL in 60 (67%) cases and the TPPA in 85 (96%) cases. All the tests were positive in 68 patients with secondary syphilis. In 72 cases of early latent syphilis, the Murex EIA screening test was positive in 68 (94%) patients, the Mercia IgM EIA in 50 (69%) cases, the VDRL in 61 (85%) cases and the TPPA in 68 (94%) cases. The Mercia IgM EIA was the only test positive in four (6%) of these cases; these four patients were known contacts. Antibody titres in the VDRL and TPPA increased as the infection progressed.
Introduction
Most laboratories in the UK use an antitreponemal enzyme immunoassay (EIA), or a combination of the Treponema pallidum haemagglutination assay (TPHA) (or particle agglutination assay [TPPA]) and the Venereal Diseases Research Laboratory (VDRL) test (or rapid plasma reagin test [RPR]), for serological screening of syphilis. The screening antitreponemal EIA, the VDRL and the TPHA, however, may be negative during early stages of infection. Antitreponemal IgM is produced early in the course of syphilis, 1 and it might be expected that an antitreponemal IgM test would be more sensitive than the VDRL and TPHA/TPPA in the diagnosis of primary infection. Although the TPPA appears to be more sensitive than the TPHA in the diagnosis of primary syphilis, 2 there are few reports on its performance when measured against an antitreponemal IgM test.
The aim of the present study is to evaluate the use of various serological tests, including an antitreponemal IgM test, in the diagnosis of early syphilis. As little has been published on the quantitative aspects of the serological reactivity in the VDRL test and the TPPA, a further aim is to explore the relationship between the stage of early syphilis and antibody titres using these tests.
Methods
Serological tests for syphilis were undertaken on all new or ‘return new’ patients who attended the Department of Genitourinary Medicine, Edinburgh Royal Infirmary between 1 January 2001 and December 31 2006.
Patients
Two groups of patients in whom syphilis was diagnosed or who were at risk of infection were studied: (1) patients who were named contacts of individuals with early, infectious syphilis and (2) all men and women who had not been treated previously, but in whom a diagnosis of early syphilis was made. Study patients were identified from the clinic database, and their case records were retrieved. Note was made of the stage of syphilis at the time of diagnosis, and if primary, the duration of symptoms prior to clinic attendance. It was also noted whether or not they had been tested for HIV infection, and if they were infected, the CD4+ T-cell count at the time of serological testing for syphilis.
Early syphilis comprised primary, secondary and early latent infection. Primary syphilis was defined as the tissue reaction to the inoculation of treponemes, and hence the appearance of anogenital or oropharyngeal ulceration in the absence of generalized skin lesions or other evidence of secondary syphilis. In some cases, dark-field microscopy and/or a polymerase chain reaction to detect T. pallidum was undertaken to confirm the clinical diagnosis. Secondary syphilis was diagnosed when the recognized clinical features were present. Early latent syphilis was defined as positive serology (antitreponemal EIA, TPPA, VDRL and/or antitreponemal IgM EIA) in the absence of clinical signs of infection in patients who had had negative serology within the preceding two years or were known to have had recent sexual contact with an individual being infected with syphilis.
Laboratory methods
All patients were screened for syphilis using the Murex ICE EIA (immune capture enzyme immunoassay), which detects both IgG and IgM antibodies. A complete confirmatory test profile was performed on sera that gave a positive EIA (or an antibody index within 10% of the cut off) on screening, as well as on sera from sexual contacts of patients with syphilis, and those with clinical signs of syphilis whenever these were requested clinically. Heat-inactivated serum was used for the confirmatory testing that comprised: a quantitative VDRL carbon antigen test, a quantitative TPPA test, and the Mercia syphilis M EIA specific for antitreponemal IgM.
Statistical tests
Data were entered into Statgraphics® statistical software (Statgraphics; Manugistics, Rockville, MD, USA). The Mann-Whitney U and χ2 tests were used in the analysis of parametric and categorical data, respectively. Linear regression analysis was used to detect the correlation between the VDRL titre and the duration of the primary lesion of syphilis.
Results
The percentage reactivity of the Murex EIA screening test, the VDRL, TPPA and Mercia IgM EIA in primary, secondary and early latent syphilis is shown in Figure 1. All the tests showed 100% reactivity in secondary syphilis. TPPA showed the highest reactivity of the tests in primary infection (96%), whereas the EIA screen and TPPA were of equal reactivity (94%), in early latent infection.

Reactivity of tests in early syphilis. EIA=enzyme immunoassay, VDRL=Venereal Diseases Research Laboratory, TPPA=Treponema pallidum particle agglutination assay
Group 1
Serological tests in sexual contacts of individuals with early, infectious syphilis
Sixty-seven patients (63 men and four women) attended as sexual contacts of a partner with early syphilis. All the serological tests were negative in 46 patients; none of them were treated previously for syphilis. In the remaining 21 cases (one man had been treated previously for early latent syphilis); none of them had clinical features of early infection. The Murex EIA screening test was positive in 17 men. In each case, the Mercia IgM EIA, the VDRL and the TPPA were also positive. Of the four men who had a negative-screening EIA, only the antitreponemal IgM test was positive. Seroconversion in the VDRL and TPPA tests was noted in one of these four patients who were retested after treatment; these tests remained negative in the remaining three cases.
Group 2
Primary syphilis in previously uninfected patients
Eighty-nine patients (85 men and four women) had primary syphilis, the clinical diagnosis being confirmed using dark-field microscopy and/or polymerase chain reaction in 20 of the 33 patients in whom these investigations had been undertaken. Figure 1 shows the reactivity of the serological tests in primary infection, whereas Figure 2 shows the pattern of reactivity for the IgM EIA, VDRL and TPPA tests in patients who responded with positive and negative EIA screening tests. All serological tests were negative in one case (1%). The Murex EIA screening test was positive in 67 (75%) patients, the VDRL in 60 (67%), the TPPA in 85 (96%) and the Mercia IgM EIA was positive in 80 (90%) cases. Repeat serological testing of five men who had an initially negative antitreponemal IgM test showed conversion to positivity in blood taken from three of these men eight, 11 and 18 days later, respectively; the VDRL remained negative in two of these men. Two of three men whose initial TPPA was negative showed seroconversion. Seroconversion in the VDRL test and TPPA was noted in one of two men during follow-up after treatment. In two cases only the Murex IgM EIA was positive; seroconversion in the VDRL test and TPPA was noted during follow-up after treatment.
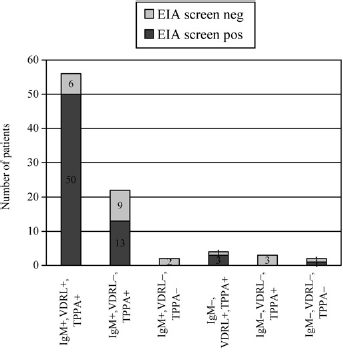
Patterns of serological tests in 89 patients with primary syphilis. IgM=Immunoglobulin M, VDRL=Venereal Disease Research Laboratory, TPPA=Treponema pallidum particle agglutination assay
Figure 3 shows the VDRL titres in the different stages of early syphilis. The VDRL titres in primary infection, median 8 (range 1-64) were significantly lower than in secondary syphilis (median 32, range 4-512; P < 0.001). TPPA titres were also significantly lower in primary infection than in secondary infection (Figure 4); only 45% of cases of primary infection had a TPPA titre 7gt;640 when compared with 100% of cases of secondary syphilis (P < 0.0001).
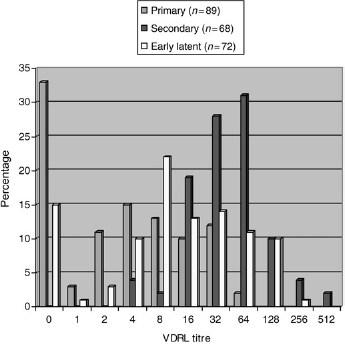
Serum Venereal Diseases Research Laboratory (VDRL) test titres in different stages of early syphilis

Serum T. pallidum particle agglutination assay (TPPA) titres in different stages of early syphilis
The median duration of the primary lesion in the 84 patients in whom it had been recorded was 14.0 days (interquartile range 13.5 days). There was a weak correlation between the VDRL titre and the duration of the lesion (R2 = 17%; P = 0.04). The longer the duration of the primary lesion, the more likely was the Mercia IgM EIA to be positive. The median duration of the lesion in those with a positive test result was 14 days, compared with seven days in those with a negative test (P < 0.001). Higher titres were noted in the TPPA in patients whose primary lesion had been present for more than 14 days (21/33 patients had a titre >640) than in those in whom it had been present for a shorter time (18/51 patients had a titre >640) (χ2 = 5.38; P = 0.02).
The HIV status of 70 patients was known: 11 were HIV-infected, the median CD4+ T-cell count being 434/mm3 (range 222-938). The Murex screening EIA was positive in eight of the 11 cases, the Mercia IgM EIA in eight cases, the VDRL positive in six men and the TPPA positive in 10 men. There was no significant difference in the seropositivity rate in the Murex screening EIA, and in the Mercia IgM EIA between HIV-infected (eight of 11 and eight of 11, respectively) and non-infected individuals (44/59 and 53/59, respectively); χ2 = 0.02 and 1.13, respectively (in each case P > 0.05). There was no significant difference in the median VDRL titre between HIV-infected (median 2) and non-infected patients (median 4) (P > 0.05). The proportion of HIV-infected individuals with a TPPA titre ≥5120 was similar to that of HIV-non-infected individuals (four of versus 16/59; χ2 = 0.07; P > 0.05).
Secondary syphilis in previously uninfected patients
Sixty-eight patients (67 men and one woman) had secondary syphilis. The Murex EIA screening test, the Mercia IgM EIA, the VDRL and the TPPA were positive in all the patients (Figure 1). In patients with secondary syphilis, higher titres were found in the TPPA than in those with primary infection (Figure 4).
The HIV status was known in 58 patients: 17 were HIV-infected the median CD4+ T-cell count being 380/mm3 (range 178-818). There was no significant difference in the median VDRL titres between HIV-infected and uninfected individuals: 32.0 and 64.0, respectively (P > 0.05). TPPA was positive in all cases; the titre was ≥5120 in 14 patients. There was no significant difference in the proportion of patients with a TPPA titre ≥5120 between those who were infected with HIV and those who were not (χ2 = 1.42; P > 0.05).
Early latent syphilis in previously untreated patients
Seventy-two patients (70 men and two women), including the 20 who were named contacts of individuals with early syphilis, had early latent syphilis. Figure 1 shows the reactivity in the serological tests. In 68 cases (94%), both the Murex screening EIA and the TPPA were positive; in the other four patients, all known contacts (see above), only the Mercia IgM EIA was positive. Both the antitreponemal IgM EIA and the VDRL tests were positive in 44 cases; in six men, the IgM test was positive, but the VDRL test was negative. Conversely, 17 patients had a positive VDRL, but negative IgM EIA; in five cases both the VDRL and IgM EIA were negative.
Figure 3 shows that the VDRL titres in early latent infection were higher than in primary syphilis, but lower than in secondary infection (The median VDRL titre [8, range 0-256] was significantly greater than that in primary syphilis [P < 0.001], but less than that in secondary infection [32, range 4-512] [P < 0.001]).
The HIV status was known in 58 patients: five were HIV-infected, the median CD4+ T-cell count being 394/mm3 (range 250-400).
Discussion
The importance of selecting a battery of serological tests in known sexual contacts of individuals with infectious syphilis is shown in this study. Almost 20% of infected contacts would not have been identified if the screening EIA was used alone. In all cases, either the TPPA or the antitreponemal IgM test or both were positive and no additional infections were identified in the VDRL test. Small numbers of patients, however, preclude the drawing of further conclusions on the value of testing contacts by the latter test.
The diagnosis of primary syphilis can be difficult. Although dark-field microscopy is a highly sensitive test when performed by skilled personnel, 3 this method requires an experienced operator, and is labour-intensive; in addition, this investigation is of limited value in the diagnosis of primary infection at extra-genital sites. Molecular tests for T. pallidum-specific DNA such as a PCR are available, 4 but generally used only in larger centres. Serological tests, therefore, remain the most important tool for the diagnosis of primary syphilis. The Murex EIA used for screening failed to identify almost one-quarter of the present cases. Similar data were presented by Wheeler et al. 3 It has been known for many years that the VDRL test lacks sensitivity in detecting primary syphilis,5,6 and in the present series the test was negative in about one-third of patients. Antitreponemal IgM is produced early in infection, and it would have been thought likely that a test for this antibody would be highly sensitive. However, despite performing better than the screening EIA and the VDRL, the test was negative in 16% of cases, a finding similar to that reported by others.7,8 There appeared to be a relationship between the duration of the lesion and reactivity in this test. However, three men whose initial antitreponemal IgM test was negative seroconverted some days later. Quality control, particularly of IgM tests is essential, as shown in the study by Muller et al., 9 who presented the results of a quality control survey of serological testing for syphilis in German laboratories. They showed that almost 5% of results in an EIA for IgM were false-negative.
In the present series of cases, and in those of others, 10 the TPPA was the most sensitive test for primary infection, being positive in 94% of cases. There was evidence of a weak association between the reactivity in the VDRL and the duration of the primary lesion, and the longer the duration of the lesion, the more likely it was to have a positive Mercia IgM EIA. Higher titres in the TPPA were more likely in patients whose lesion had been present for more than 14 days. These findings are not unexpected as serum antibody titres progressively increase as infection progresses. 1 It is clear that when a diagnosis of primary syphilis is being considered clinicians should alert the laboratory, so that additional serological tests may be performed.
Capture EIA is a very specific method for detecting antitreponemal IgM, 7 however, false-positive reactions have been described, particularly in the presence of rheumatoid factor. 8 In the present study, only the Mercia IgM EIA was positive in six patients - four were sexual contacts of known infected partners and two had proven primary infection. Seroconversion in other serological tests was noted in the two cases of primary infection and in one of the four sexual contacts, providing evidence for the specificity of the test in these patients. In the other three patients, however, false-positive reactions cannot be entirely excluded.
In patients with secondary syphilis, the Mercia IgM EIA performed better than the previously reported data for EIAs. Ijsselmuiden et al. 7 noted that only 12 of 20 sera samples from patients with secondary syphilis were reactive in a capture EIA. In another small series of patients with secondary infection, Lefevre et al. 8 found that only 11 of 13 sera were seropositive in the Mercia IgM EIA. Titres in the VDRL test were significantly higher than those in primary syphilis, as were those in the TPPA.
In the diagnosis of early latent syphilis, the Mercia IgM EIA was the least sensitive test, being positive in only 69% of cases. This finding is in keeping with the finding in animal models in whom serum IgM titres fall as the duration of the infection increases. 1 As discussed above, however, the test was useful in detecting infection in contacts. The TPPA only failed to identify infection in those with very early latent infection (four cases). Apart from these four cases, the TPPA was positive, generally at high titres: in 74% of all cases of early latent infection, the titre was ≥5120.
In this small series of cases, HIV infection did not appear to influence the serological response in any of the tests. There was no significant difference between the median VDRL titres in patients with primary and secondary syphilis. This finding, however, contrasts with that of Rompalo et al. 11 who noted significantly lower and higher RPR titres in patients with primary and secondary syphilis, respectively. Small numbers of HIV-infected patients in our study, however, may have masked an HIV effect.
In conclusion, the Murex screening EIA is an effective tool for the diagnosis of early syphilis beyond the primary stage in patients who have not previously been treated for this infection. This also seems to hold true for infection in HIV-infected individuals. TPPA and/or Captia IgM were positive in all cases of primary infection. When primary infection is suspected, the importance of ordering these additional tests should be borne in mind by the clinician. It should also be borne in mind that not all EIAs used for screening or detecting specific antitreponemal IgM will have the same performance characteristics as those used in this study.
Footnotes
Acknowledgements
We wish to thank the staff in the Syphilis Specialist laboratory for performing the various serological tests reported in this study.