
Abstract
Summary:
The Sexually Transmitted Infection Foundation course (STIF) is a recommended training course for UK general practitioners (GPs) and others delivering sexual health services in the community. We assessed the impact of attending the course on testing for HIV and chlamydia. Thirty-one GPs attending Brighton STIF courses were identified and the laboratory database was searched to identify all chlamydia and HIV tests they requested in the three months prior to attending, the first three months after attending and the subsequent three months. Three hundred and eight chlamydia tests were performed precourse, 390 postcourse and 342 in the following three months. This represented a significant increase from baseline to postcourse (P = 0.007), which was lost by three to six months (P = 0.25). The proportion of positives did not change. A total of 98, 111 and 131 HIV tests were performed in the three time periods of which; none were positive. Barriers other than training may need to be overcome to increase HIV testing in primary care.
Introduction
Diagnoses of sexually transmitted infections (STIs) and HIV have increased in the UK in recent years. 1 This increasing demand, alongside government policy, such as the National Strategy for Sexual Health and HIV, is changing the delivery of sexual health services. 2 A shift of emphasis to primary care has been encouraged to achieve government objectives and increase capacity to achieve targets, e.g. screening 50% of the sexually active population annually for chlamydia, 3 and to diagnose infections promptly, thereby avoiding consequences of late diagnosis (e.g. increased mortality with HIV 4 and infertility with chlamydia 5 ). Barriers to achieving this include general practitioner (GP) time, 6 lack of resources and training. 7 The Sexually Transmitted Infection Foundation (STIF) course, designed by the British Association for Sexual Health and HIV (formerly the Medical Society for the Study of Venereal Diseases), is a medium to address this training issue and has been implemented since 2002 across the UK. We set out to devise and apply a quantitative and practical method to assess the impact of the STIF course on GP testing for chlamydia and HIV in the area served by our genitourinary (GU) medicine clinic.
Methods
Eligible GPs were those who had attended a STIF course locally and had a unique identifying code in our microbiology laboratory. The numbers of tests (and results) for chlamydia and HIV were determined by searching the laboratory database for three time periods: three months prior, 0-3 months post and 3-6 months postattendance on the STIF course. The data were analysed in SPSS 12.0.1 using the Friedman test and Wilcoxon's signed rank test. The proportion of tests positive at each time point was compared with a χ2-test. To control for unrelated changes in testing over time, the precourse testing rates from GPs on consecutive courses were compared using the Kruskal-Wallis test. Ethics committee approval was not required for this study.
Results
Between April 2002 and 2004, five STIF courses took place with a total of 214 participants. Fifty-seven GPs attended. Thirty-one met the inclusion criteria.
There was no significant difference between GP cohorts in either chlamydia (P = 0.230) or HIV (P = 0.603) testing at baseline.
The numbers of chlamydia tests performed in the three time periods were 308, 390 and 342, representing a significant increase in the three months immediately postattendance (*P = 0.007) with a non-significant fall in the subsequent three months (**P = 0.13) (Figure 1). There was no change in the proportion of positive tests with 4.22%, 2.82% and 4.68%, respectively (P > 0.10, χ2 = 2.88, df = 2).
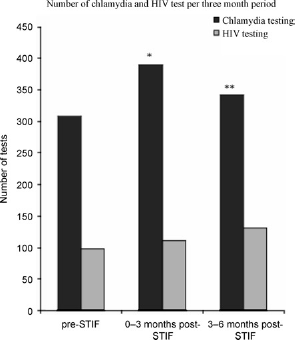
Number of chlamydia and HIV tests per threemonth period
The numbers of HIV tests performed in the three time periods were 98, 111 and 131 (P = 0.59 and 0.37, respectively). None were positive.
Discussion
Where previous studies have assessed changes in knowledge 8 and self-reported practice 9 after an STI training intervention, we have attempted to assess an intervention in terms of the number of tests performed.
The method used is easy to apply and provides useful information. GPs were not aware of the study, avoiding potential bias and the workload of staff was unaffected. Limitations include the potential use of the laboratory code of a GP by other staff and the lack of denominator; we do not know how many opportunities to test were missed or whether testing is targeted appropriately or was offered and refused. In addition, as this is an optional course, we may be ‘preaching to the converted’, although 3-400 chlamydia tests performed in three months by 31 GPs seems well below the screening targets.
The early increase in chlamydia testing was not sustained. This suggests that the STIF course is effective in changing practice in the short term and implies that a follow-up intervention may be necessary to sustain the effect.
The proportion of positive chlamydia tests remained stable and low when compared with the local chlamydia screening programme, which has a positive rate of 9.8% (Elizabeth Ambler, 2007, personal communication). This may be due to differences in the age range of the populations being screened in the two programmes as it has been previously documented that the majority of chlamydia screens in primary care were in women over 25 years, however, the age of those tested was not available. 10
HIV testing did not significantly increase and no HIV tests were positive. A number of possible explanations may be suggested, e.g. training is not the most important barrier to HIV testing in primary care, the STIF course does not sufficiently cover HIV testing (unlikely, as considerable time is devoted to this) or the issue is raised by GPs, but patients prefer to test in GU medicine. It is possible that GPs may not attend patients at risk of HIV, but these data could support assertions that HIV is often missed in this setting. 4
Further study to identify methods of sustaining increased testing and understand barriers to HIV testing will be required if we are to succeed in increasing the role of primary care in sexual health. Improved methods of assessing the practical outcomes of educational interventions are needed to ensure the delivery of course aims and objectives.
Footnotes
Acknowledgements
We are grateful to the participants in the STIF courses studied and to Matthew Longbone, Microbiology data manager, for his help in collecting the data.