
Abstract
Consistent condom use can prevent sexually transmitted infections (STIs), but few studies have measured how the prevalence of consistent use changes over time. We measured the prevalence and correlates of consistent condom use over the course of a year. We did a secondary analysis of data from an HIV prevention trial in three sexually transmitted disease clinics. We assessed condom use during four three-month intervals for subjects and across their partnerships using unconditional logistic regression. Condom use was also assessed for subjects during all three-month intervals combined. The 2125 subjects reported on 5364 three-month intervals including 7249 partnership intervals. Condoms were always used by 24.1% of subjects and 33.2% of partnerships during a three-month interval. Over the year, 82% used condoms at least once but only 5.1% always used condoms. Always use of condom was more likely for subjects who had sex only once (66.5%) compared with >30 times (6.4%); one-time partnerships (64.1%) compared with main partnerships (22.2%); and in new partnerships (44.0%) compared with partnerships that were not new (24.5%). Although consistent condom use may prevent STIs, condoms were rarely used consistently during the year of follow-up.
Keywords
INTRODUCTION
There is considerable debate on the effectiveness of condoms for preventing sexually transmitted infections (STIs) including HIV. 1–3 Individuals who use condoms consistently and correctly reduce their risk of infection because STI cannot pass through latex condoms. 4 However, at the population level, the effectiveness of consistent condom use will depend on how many people use condoms consistently.
Condom use has been measured dozens of ways with different partner specifications, response alternatives and recall periods (usually a few months or less). 5,6 Studies suggest that at least use of condoms has increased to a certain extent. Condom use during the last episode of sex increased from 46.2% in 1991 to 63.0% in 2003 among adolescents in the USA. 7 Studies of consistent condom use often report on different time intervals. Condoms were used consistently among persons who were sexually active: for six months by 56–75% of young men in Kampala, Uganda; 3 for three months by 35% of females who attended an adolescent health clinic in Atlanta, GA, USA; and for one month by 46% of young women who attended an STI clinic in Birmingham, AL, USA. 8 Only a few studies report on consistent condom use over multiple intervals. In a community randomized trial in Rakai, Uganda, condoms were used consistently for 12 months by 3% of participants at baseline, and for 10 months by 5% of participants during the second follow-up visit. 9,10 In a circumcision trial in Rakai, consistent condom use over the interval was reported by 18% at six months, 18% at 12 months and 19% at 24 months. 11 Neither of these studies reported whether the consistent users from one interval continued to be consistent users in the next interval. In fact, we are unaware of any studies that have evaluated changes in consistent condom use in a large population over time.
We studied condom use in a group of persons followed for a year after visiting an STD clinic. Our goal was to determine how often condoms were used consistently over time and to identify factors associated with consistent use.
METHODS
We conducted a secondary analysis of data from RESPECT-2, a randomized controlled trial of HIV prevention counselling conducted in three public STD clinics in Denver, CO, Long Beach, CA, and Newark, NJ, USA. 12 Eligible clients visited the clinics for a complete diagnostic STD examination, were HIV-negative at enrolment, reported vaginal or anal sex in the preceding three months, and were aged 15–39 years. At the initial visit participants were counselled, examined and tested for STDs and HIV. In addition, half of the participants received additional counselling at the 6-month visit to test the effects of a booster counselling session. 13 Counsellors encouraged clients to identify and commit to a single step to reduce their STI/HIV risk. Some clients chose plans related to condom use while others focused on limiting partners or changing other risk behaviours. Outcomes were measured three, six, nine and 12 months from the date of enrolment. Condom use did not differ by intervention arm, so we did not adjust for intervention arm in the analysis. This analysis was limited to heterosexuals who had a clinic visit both immediately before and after a three-month interval. For example, a subject who returned at three, nine and 12 months would contribute data from baseline to three months and from nine to 12 months.
Behavioural data were collected using audio computer-assisted self-interview at enrolment and at each scheduled follow-up visit with a three-month recall period. The study questionnaire contained detailed information on up to three different sex partners; we excluded intervals where a subject reported more than three sex partners because we did not have data on condom use with each partner. For each partner, subjects were asked to report the number of times they had vaginal sex and the number of times they used a condom. Condom use was then classified as always (100%), never (0%) or sometimes (all numbers in between).
We first analysed condom use by subject, which included all of the partnerships that a subject reported in each three-month interval. Predictors of always using condoms were identified using unconditional logistic regression. Generalized estimating equations were used to account for within-subject correlation of repeated measures. 14 Several correlation structures were assessed and provided very similar results, so we show only the results of exchangeable structures.
Analyses of condom use within partnerships used the same methods described above. This analysis included up to three partners per subject for each of the four three-month intervals, so each subject could report on up to 12 partnerships.
Condom use was also assessed across multiple intervals for subjects who returned for either three or four follow-up visits. (Partnerships could not be reliably linked across intervals, so this analysis could not be done for partnerships.) Unconditional logistic regression was used to measure the association between characteristics of the subjects and condom use. Associations with condom use were similar to associations from the three-month interval analyses, so these data are not shown.
RESULTS
RESPECT-2 enrolled 3297 subjects, of whom 2868 (87.0%) returned for at least one follow-up visit. After excluding 159 who self-identified at baseline as men who had sex with men, 376 who had no intervals with both before and after visits with laboratory tests, and 208 who had no intervals with one, two or three sex partners, there were 2125 subjects who reported their behaviour during a total of 5364 three-month intervals. Subjects reported on sexual behaviour and condom use from one interval (25.7%), two intervals (26.0%), three intervals (18.5%) or all four intervals (29.8%). Subjects could report on up to three partnerships per interval; the total number of partnership intervals was 7249.
Condoms were always used by 24.1% of all subjects and in 33.2% of all partnerships during a three-month interval. However, among the 647 subjects followed for all four intervals, only 5.1% always used condoms throughout the year (Figure 1). Never using condoms followed a similar pattern. Condoms were never used by 36.8% of subjects or in 40% of partnerships during a three-month interval. However, for those sexually active subjects followed for four intervals, only 17.9% had never used a condom. Many subjects changed their condom-use over time. For example, after four three-month intervals, 68.3% had been in different condom-use categories for at least two intervals.
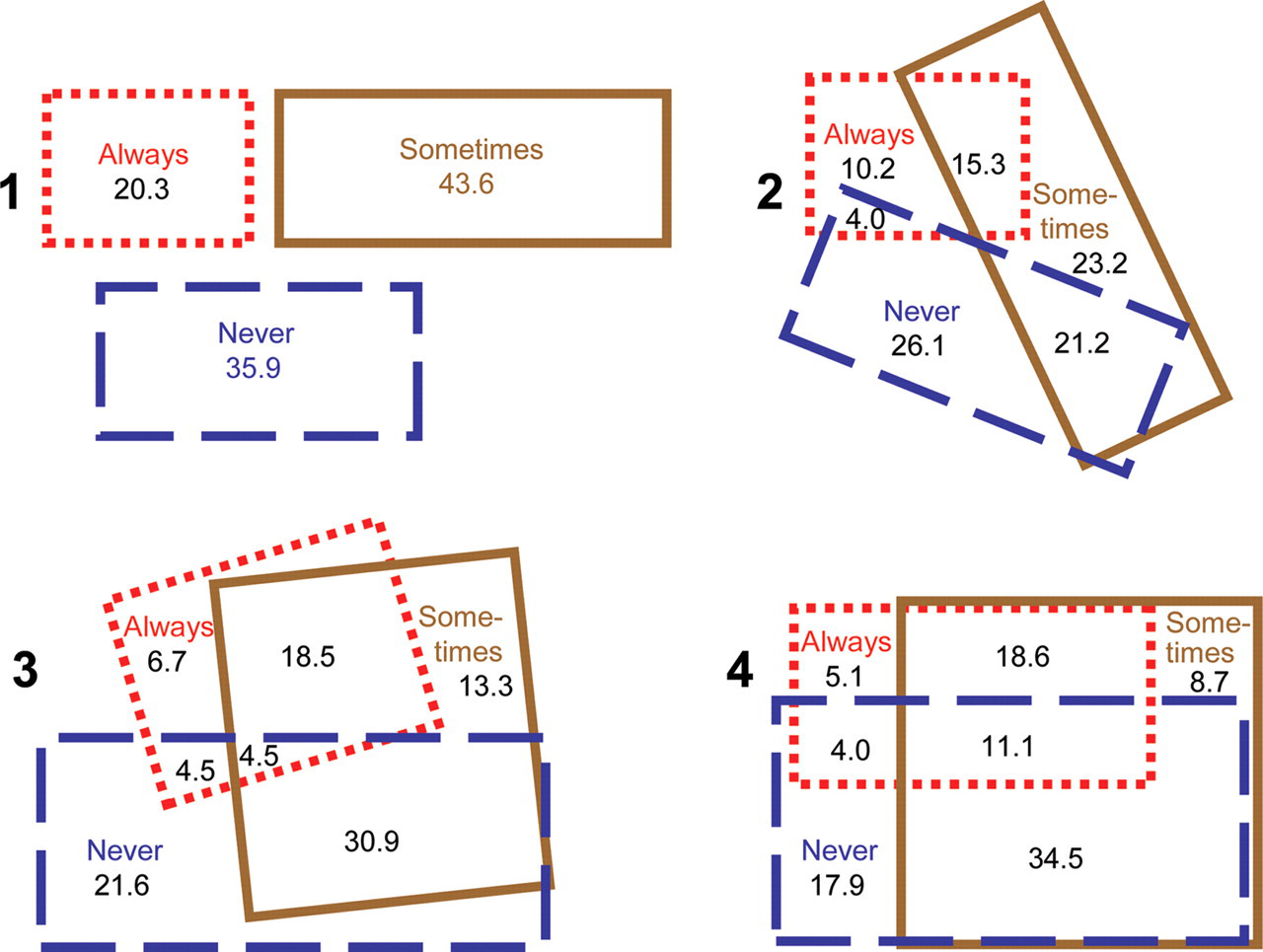
Overlap of condom use during one, two, three or four three-month intervals. After one interval, subjects' condom use was neatly classified as always, sometimes or never. Over time, subjects moved from one category to another. For example, after two intervals, 15.3% of subjects had used condoms always in one interval and sometimes in another interval. After three intervals, 4.5% of subjects had used condoms always in one interval, sometimes in another and never in the third interval
The number of sex acts was the strongest determinant of condom use in the interval. A subject who had sex only once was 10 times more likely to always use condoms compared with a subject who had sex more than 30 times during a three-month interval (Table 1). As the number of partners increased, the likelihood of always using condoms decreased from 25.7% of subjects with one partner to 16.0% of subjects with three partners (adjusted odds ratio 0.44). Main partnerships were less likely to always use condoms (22.2%) than one-time partnerships (64.1%) or other partner types (48.0%) (Table 2). Sex in new partnerships (they had sex for the first time within the past three months) was more likely to be always protected by a condom (44%) compared with sex in partnerships who were not new (24.5%) (Table 2). Also, the more new partners a subject had, the more likely they were to always use condoms (Table 1). This contrasts with the finding (above) that subjects with more total partners were less likely always to use condoms.
Subjects' condom use during three-month intervals, by subject characteristics
Odds ratios are adjusted for all the variables in the table
n is the number of three-month intervals for the subjects with each characteristic
CI = confidence interval; STD = sexually transmitted disease
Partnerships' condom use during three-month intervals, by partnership characteristics
Odds ratios are adjusted for all of the variables in the table
n is the number of three-month intervals for the partnerships with each characteristic
CI = confidence interval; STD = sexually transmitted disease
Other variables were only weakly associated with always using condoms. Partnerships with younger partners were slightly more likely to use condoms always than partnerships with older partners (Table 2). Males were slightly more likely to report always using condoms compared with females during a three-month interval (Table 1). When subjects reported that one of their partners was considered ‘very likely’ or ‘likely’ to transmit an STI if they had sex without a condom, always use of a condom increased only slightly and the increases were not statistically significant (Table 2).
Some variables that one might expect to be related to condom use were not. For example, subjects who were treated for an STI at their last clinic visit were no more likely to use condoms always than subjects who were not treated for an STI (Table 1). Condom use was also not strongly associated with clinic, race, study interval or subject's age (Tables 1 and 2).
Subjects were not asked about why they used condoms, but they were asked about the last time they had sex without a condom. Among subjects who sometimes used condoms, the most commonly reported reasons for not using a condom were: ‘we had sex in the heat of the moment’ (30%); ‘I didn't think that I would get an STD or AIDS from him (her)’ (25%); ‘I knew he (she) was HIV-negative’ (22%); and ‘already using birth control’ (17%). Subjects who sometimes used condoms rarely reported ‘I didn't want him (her) to think I didn't trust him (her)’ (2%) or ‘I didn't want him (her) to think he (she) couldn't trust me’ (3%).
DISCUSSION
In this STD clinic population, almost all (82%) subjects followed for a year used a condom at least once but almost all condom users (94%) also had sex without a condom at least once (Figure 1). Although some condom use was very common, consistent condom use over time was very rare. Thus, in this population of patients at risk for STD, there is little need for interventions to promote trying condoms, but there is a major need for interventions to promote consistent use.
The number of times sex was reported within a partnership was the strongest determinant of consistent condom use. Consistent condom use over three months was reported for two-thirds of partnerships who had sex once, half of partnerships who had sex two to five times, and only one-quarter of partnerships who had sex six to 10 times. This rapid decline in consistent condom use suggests either most subjects were not committed to consistent condom use over time, or that the commitment was not maintained. It also demonstrates that studies of condom effectiveness should adjust for the number of sex acts because persons reporting 100% condom use will likely have had many fewer sex acts than persons reporting less than 100% condom use.
Most of the persons in this study appeared to be using condoms as a part of an STD/HIV risk-reduction strategy. Subjects were more likely to use condoms consistently with one-time or other partners compared to main partners, and with new partners compared to old partners. This suggests that people often discontinue condom use when they believe they are at low-risk for an STI. The pattern of high condom use early in a relationship followed by decreasing use over time was described in 1994 as the ‘sawtooth’ approach. 15 Other recent studies have found rapid declines in condom use among adolescents, from 66% using condoms at the beginning of a relationship, to only 43% consistently using them three weeks later. 16 Furthermore, the sometimes users of condoms often reported the reason for not using a condom was because they thought they were at low-risk for acquiring HIV or another STD. Similar associations with condom use have also been found in other studies. 17–19 Many subjects appeared to use condoms for STI/HIV prevention when they thought their partner might be infected, but their use was often inadequate.
We did not compare infection rates for condom users and non-users because we did not know whose partners were infected (or when). With no information on infection among partners it is impossible to know which subjects reduced their STD risk using condoms, and thus we cannot estimate the STD-prevention benefit from condom use in our population. However, 18% of our study population acquired one or more STI during a year of follow-up 12 suggesting that condom use was not good enough. Although some of those infections may have been due to condom failure, most appear to have been due to failure to use condoms when having sex with an infected partner. With only 5% of the population using condoms consistently during the year, the number of participants protected by consistent condom use is very small. Even the consistent condom users may have been exposed to STI if condoms broke, slipped off or were not used correctly. 18,20–23
Effectiveness in the use of condoms could be improved by increasing its use in general or by increasing its use specifically with partners likely to be infected. Our study suggests that subjects thought their partners were safe after they had sex a few times or when they were considered to be a main partner. However, STI are often asymptomatic, and even bacterial infections may persist for many months, 24 so condom use must continue until a monogamous partner has negative tests for STI.
Our study has some limitations. Although we asked subjects why they stopped using condoms, we did not ask why they started using condoms. Condoms may have been used at the beginning of a relationship for reasons only tangentially related to STD, such as to demonstrate respect and concern for a new partner. We asked people about their condom use over a three-month period and some error in recall is likely, probably leading to overestimates of consistent condom use. We included persons who had visited STD clinics and enrolled in a trial requiring four follow-up visits over a year, so our findings may not be generalizable to other populations. Subjects received STD prevention counselling, so condom use was probably higher than in other populations. We did not ask subjects if they stopped using condoms after they and their partners were tested for STI, and we could not tell who had infected partners, so we could not identify persons who really needed condoms for STI prevention.
Consistent and correct condom use can prevent STIs for persons who choose to be sexually active. We found that condoms were commonly used but consistent condom use was rare in this population at high-risk for STI. Many persons used condoms for STI prevention; however, condoms are unlikely to prevent STI in partnerships in which they are only sometimes used. 10 Additional research is needed to identify reasons why individuals use condoms at the very beginning of a relationship but stop later on. Interventions are needed to help persons increase consistent condom use until they enter a mutually monogamous relationship with an uninfected partner.