
Abstract
A 36-year-old HIV-infected man presented with nonspecific gastrointestinal symptoms and weight loss. Biopsy of the duodenum and an intra-abdominal lymph node showed Histoplasma capsulatum. The diagnosis of histoplasmosis was delayed as the presentation was initially ascribed to intercurrent enteric pathogens and the patient's lifetime travel history was not obtained.
Introduction
Histoplasmosis is the most common endemic mycosis in HIV-infected individuals and disseminated infection occurs more frequently than in immune-competent individuals. 1 The gastrointestinal tract is involved in up to 90% cases of disseminated histoplasmosis; however, specific gastrointestinal features are uncommon.2–5 Symptoms such as diarrhoea and abdominal pain are nonspecific and histoplasmosis is often not considered in the differential diagnosis, particularly if the patient presents in a non-endemic area. We describe an HIV-infected patient with gastrointestinal histoplasmosis. Treatment of coexisting common gut pathogens and a lack of appreciation of the patient's life-time travel history/exposure risk led to delay in diagnosis.
Case Report
A 36-year-old white homosexual man presented with a six-month history of malaise, 15 kg weight loss, anorexia, night sweats, intermittent diarrhoea and worsening abdominal pain. He had been diagnosed HIV-1-positive 15 months earlier and had not received antiretroviral therapy (ART). On admission he was afebrile. Abdominal examination revealed left iliac fossa tenderness, no palpable mass, organomegaly or peritonism. Clinical examination was otherwise unremarkable. CD4 count = 80 cells/ μL (6% of total lymphocyte count) and HIV viral load = 22,800 copies/mL; no genotypic resistance mutations were identified. Initial blood investigations were normal with the exception of a normocytic anaemia (haemoglobin = 12.1 g/dL). A sexual health screen, including a rectal swab for Chlamydia trachomatis was negative. Stool microscopy was positive for Giardia lamblia and Cryptosporidium spp. Abdominal symptoms did not resolve following treatment with tinidazole.
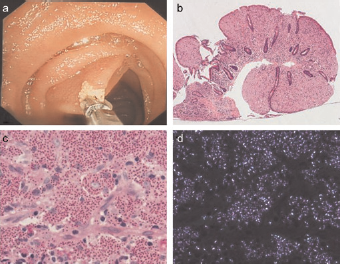
In view of the persistent abdominal symptoms, an abdominal computed tomography (CT) scan was performed. This showed extensive mesenteric and para-aortic lymphadenopathy together with jejunal wall thickening (Figure 1a and b); there was no hepatosplenomegaly. A thoracic CT scan showed multiple 2–3 mm pulmonary nodules in both apices. These features were not consistent with the microbiological diagnosis and suggested additional pathology. Upper gastrointestinal endoscopy, using a paediatric colonoscope inserted 40 cm distal to the duodenojejunal junction, showed several plaque-like lesions with normal surrounding mucosa in both duodenum and jejunum; a duodenal lesion was biopsied (Figure 2a). An ultrasound-guided intra-abdominal lymph node core biopsy was also performed. The patient declined a bone marrow aspirate and trephine. Histology of duodenal and lymph node biopsies showed histoplasmosis (Figure 2b–d); Histoplasma capsulatum was cultured subsequently from both biopsies. Blood cultures were negative. At this stage, two weeks after the initial presentation, additional history revealed that the patient was born in Europe but subsequently lived in South America for over a decade before returning to Europe for the last two decades. He last visited South America two years before this presentation.
(a) Axial intravenous contrast-enhanced computed tomography (CT) image through the lower abdomen which shows mixed attenuation mesenteric lymphadenopathy (white arrows). (b) Axial intravenous contrast-enhanced CT image through the upper abdomen showing jejunal wall thickening (white arrows), which is apparent despite collapse of small bowel loops. (c) Axial intravenous contrast-enhanced CT image through the lower abdomen which demonstrates partial resolution of previously noted lymphadenopathy (white arrows). The small bowel is now dilated. (d) Axial half Fourier Acquisition Single shot Turbo spin Echo (HASTE) MR image through the lower pelvis acquired 40 minutes after oral ingestion of 1000 mL of 0.2% locust bean gum with 2% mannitol solution. There is a short tight ileal stricture (black arrow) with upstream small bowel dilatation. There is a lack of soft tissue thickening at the stricture site. (a) Image obtained at endoscopy, showing a duodenal plaque-like lesion, with macroscopically normal surrounding mucosa. (b) The duodenal biopsy shows markedly abnormal mucosa with widespread blunting of villi and loss of duodenal crypts. Haematoxylin & eosin stain; original magnification = ×40. (c) The lamina propria is expanded by an infiltrate of macrophages, each containing numerous ovoid organisms. These organisms are periodic acid Schiff stain positive and each is circumscribed by a clear halo. Ziehl-Neelsen staining is negative; original magnification = × 200. (d) The organisms show weak birefringence under polarized light.
Oral itraconazole was commenced with rapid improvement in symptoms. ART (zidovudine, lamivudine and tenofovir) was initiated two weeks later. Choice of ART regimen was determined by lack of resistance mutations, low viral load and a wish to avoid drug–drug interactions between itraconazole and protease inhibitors or non-nucleoside reverse tran-scriptase inhibitors.
One month later, the patient presented with sub-acute small bowel obstruction. An abdominal CT scan showed improvement in jejunal mucosal thickening and partial resolution of the mesenteric lymphadenopathy (Figure 1c). MRI enterogra-phy demonstrated an obstructing short tight mid-ileal stricture without an associated soft tissue mass (Figure 1d). In the context of overall radiological improvement and lack of soft tissue component, the stricture was thought likely to be fibrotic, rather than secondary to an immune reconstitution inflammatory syndrome. The patient improved with conservative management. An elective laparatomy and bowel resection was declined by the patient, who moved abroad. Two months later, he again presented with jejunal perforation. Following emergency laparatomy and jejunal resection, the patient was doing well, 11 months later.
Discussion
This patient presented with nonspecific gastrointestinal symptoms and the diagnosis of histoplasmosis was delayed by several weeks as the presentation was initially attributed to coexisting enteric pathogens. In our patient, the abdominal CT findings prompted duodenal/jejunal endoscopy and biopsy, together with percutaneous intra-abdominal lymph node biopsy: these investigations secured a diagnosis.
Previous reports of gastrointestinal histoplasmosis in HIV-infected patients identified that ≥ 70% have symptoms of fever and abdominal pain, and ≥50% have weight loss and diarrhoea. 3,4 Gastrointestinal bleeding, bowel perforation and obstruction are less commonly described. 3,4,6 Small bowel involvement has been reported in ≥25% of HIV-infected patients with gastrointestinal histoplasmosis. 2 Jejunal strictures causing small bowel obstruction and perforation are rare.6–8
Although not unique, this case illustrates several important points for physicians caring for HIV-infected patients. With increasing international travel, HIV-infected patients may present with geographically specific diseases outside the endemic areas. Obtaining a detailed life-time travel history is crucial in facilitating consideration of uncommon aetiologies in the differential diagnosis and avoiding delay in treatment. In the HIV-infected patient more than one disease process may coexist and Occam's razor, i.e. ‘diagnostic parsimony’, frequently does not apply. Thus, identification of one pathogen should not interrupt the search for concomitant and potentially fatal pathologies. Biopsy, with both histopathological and microbiological assessment, is indicated, in order to identify and appropriately treat opportunistic pathogens.