
Abstract
Attendees at Newcastle sexually transmitted infections foundation (STIF) courses since 2002 were sent a postal questionnaire to ascertain views about the course, its effect on practice and the desire for further education. Totally 156 forms were returned (48% response). The majority 97% were satisfied with the course, 97% wanted updates, 57% annually and 33% biennially. Following a STIF course, 69% provided HIV testing (only 14% of those, prior to attendance). However, only 39% routinely offered HIV testing and only 34% routinely offered syphilis testing to patients whom they considered to be at risk of a sexually transmitted infection. Common reasons for not offering testing were lack of time for counselling, lack of confidence, no perceived need or anonymity concerns resulting in referral to genitourinary medicine. This was despite training, which encourages routine HIV testing with a pretest discussion rather than ‘counselling’ and education about recent outbreaks of syphilis.
Keywords
Introduction
The sexually transmitted infections foundation (STIF) course is a two-day course that was developed originally by the Medical Society for the Study of Venereal Diseases, now the British Association for Sexual Health and HIV (BASHH) to provide multidisciplinary training in basic recognition, understanding, management and treatment of sexually transmitted infections (STIs). 1 The target audience is doctors and nurses from primary care and family planning, genitourinary (GU) medicine, non-consultant career grade staff, health advisers and nurses, school nurses and any clinician who may encounter patients with or who has an interest in STIs. It is recommended that general practitioners (GPs) offering enhanced services for STIs in primary care attend the course. 2
A national steering group for the course provides and revises standard course materials including a CD-ROM with suggested lecture and workshop slides, instructor manual and course handbook for delegates.
Newcastle has run two STIF courses each year since 2002. The courses have always been full, 40 persons per course. The course attendees are given an assessment form at the end of each course, in which we have always scored highly consistent with national feedback data. However, we wanted to know if attendees felt they had gained long-term benefit from attending the course, especially with regards to changes in their clinical practice and their reflections on the demand for further or ongoing education.
Method
An anonymous questionnaire was sent to all delegates who had attended a previous STIF course ran by Newcastle GU Medicine Department. Questions included age, sex, year course attended, occupation and reason for attending course. They were asked specifically about the course, whether it covered their needs, its strengths and weaknesses, the value of the handbook, for the course itself and subsequently in their practice and their requirements for further education such as practical sessions and regular updates.
They were specifically asked about:
their confidence and ability in sexual history-taking since attending the course, including subsequent differences in technique; their practice with regards to testing for HIV, syphilis, chlamydia and gonorrhoea, if so to whom and any changes since attending the course.
As GPs have a lead role in primary care health provision, their responses were evaluated separately wherever relevant.
Results
General
A total of 324 questionnaires were distributed (to previous delegates with reliable contact information). One hundred and fifty-six (48%) were returned. Since three had not been completed, a total of 153 (47%) were analysed. The majority of respondents were females (90%) when compared with males 8% (2% not indicated). This is broadly a reflection of the proportion of attendees by gender. Sixty percent were aged between 36 and 50 years with 20% below 35 and 20% over 50 years of age. Fifty-four percent of the respondents were doctors, the majority (84%) GPs and 40% of the respondents were nurses. The majority of these were practice nurses (45%), family planning nurses (18%) or nurse practitioners (16%). There was a 65% response rate from delegates during the most recent courses, 2006 and 2005 respectively, compared with response ratesof 22% and 28% for the earlier courses (2002 and 2004).
The results of the main questions are shown in Table 1, although specific information was elicited as detailed below.
Responses to questionnaire
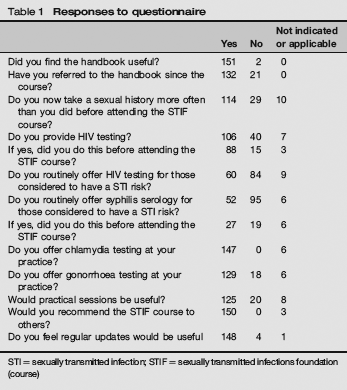
STI = sexually transmitted infection; STIF = sexually transmitted infections foundation (course)
Course handbook
Ninety-nine percent had found the handbook useful with 86% reporting that they had referred to the handbook since the course and of these 17% had used the handbook more than once a month.
Confidence in dealing with STIs following STIF course
Ninety-seven percent reported that they felt more confident in taking a sexual history with 75% (84% of GPs) stating that they did this more often than they did before attending the STIF course.
The reasons given for this were:
more confident (30% of respondents); less embarrassed; appreciation of importance following the course; more enabled and informed; increased awareness; given the skills through the course.
Greater insight into the appropriate depth and the use of key phrases in sexual history-taking was also highlighted. Those not responding positively were generally already working within sexual health including GUM and so were used to taking a sexual history on a regular basis.
HIV testing
Sixty-nine percent stated that they provided HIV testing (serology) in their clinical practice (86% of GPs) and of these 14% (14% also for GPs) had not provided this service before attending the STIF course.
Reasons given for not providing HIV testing were:
referred to GU medicine clinic for ease, full screening or confidentiality; pretest discussion, counselling and potential contact-tracing issues and concerns; no perceived need or demand; staff inadequately trained.
When asked more specifically if HIV testing was routinely offered to sexually active patients considered to be at risk of an STI, only 39% (45% of GPs) responded in the affirmative. The reasons given for not offering HIV testing included:
advised to attend GU medicine department – easier, confidentiality; insufficient time – especially for pretest discussion; other partners in practice not keen; result set-up not robust; lack of confidence despite STIF course; low prevalence in practice area, no local need, not wanted, not appropriate; never done historically; no enhanced service funding.
Syphilis testing
Only 34% (32% of GPs) of respondents routinely provide syphilis serology to those considered to be at risk of an STI, but of these 37% (61% of GPs) stated that they had introduced this service since attending the STIF course. Those not providing this service gave the following reasons:
advised to attend GU medicine department; never seen any positive serology in 25 years of practice; very rare, one positive antenatal result in 13 years as a GP; risk considered to be very low except in certain groups, but aware that bisexual/homosexuals may not be recognized by sexual history; providing serology would have massive implications for counselling, workload, funding; no local need; forgot about it, not part of repertoire.
Chlamydia testing
Although chlamydia testing is provided by 96% (100% of GPs) within their practice, 86% reported offering it to symptomatic patients and 88% (93% of GPs) to asymptomatic patients. When asked about promoting testing, 77% (70% GPs) said that they promoted opportunistic chlamydia testing in all sexually active patients less than 25 years of age as part of the national screening programme.
Gonorrhoea testing
Eighty-four percent (93% of GPs) reported offering gonorrhoea testing during their practice. Reasons given for not testing for gonorrhoea were ‘follow-up contact-tracing’, ‘if high risk or clinically suspicious I refer to GU medicine’, ‘inadequate facilities’ or ‘lack of suitable swabs’. If gonorrhoea testing was available, 31% offered it only to women, with 67% offering it to both men and women.
The course as a whole
Ninety-two percent of all respondents felt that the STIF course had covered the necessary basic information about STIs, although six respondents (4%) felt that there was not enough detail and four thought there was too much detail. Eight-two percent would have valued practical sessions with 54% specifying one or two, 34% three or four and 9% either more or unspecified. Ninety-eight percent of respondents would recommend the STIF course to others.
Course updates
Ninety-seven percent of respondents felt that regular updates after the course would be useful. Of these, 57% (48% of GPs) wanted annual updates, 33% (36% of GPs) felt biennial updates and eight percent (15% of GPs) felt triennial updates would be useful. When asked about the nature of updating material, there was an even spread of responses between a refresher STIF course, update lectures and online learning, with only 16% asking for practical sessions.
Discussion
Some caution is required in interpreting and evaluating the results of this study as it covers those attending Newcastle STIF courses from 2002 to 2006 as changes in the prevalence of infections and new developments have occurred. These include the appearance of lymphogranuloma venereum in homosexual/bisexual men, the large increase in infectious syphilis, the national roll-out of the chlamydia screening programme, the introduction of 48-hour access targets for GU medicine and associated initiatives.
This questionnaire has highlighted that most respondents (97%) felt that they needed updates following the STIF course, with the majority asking for annual or biennial updates. The altering prevalence of infections and the change in clinical practice with the introduction of new faster, non-invasive tests and new treatments reinforces the importance of updating. At the time of writing, the BASHH STIF Steering Group has recognized this and is in the process of formulating update modules and advising on course updates. Our respondents wanted a variety of media for updates, including online learning, lectures and practical sessions. The majority of respondents felt that practical sessions following the STIF course would have been useful and this is something which should be explored. However, the practicalities of arranging these sessions and charging for training would have to be considered. Most respondents requested one or two practical sessions. An alternative may be a simulated workshop.
It is reassuring that 75% were taking a sexual history more often since attending the STIF course; this increase has been identified in a similar study. 3 The sexual history is the crux of sexual health assessment, identifying risks, necessity for testing and health promotion. However, there is little point in taking more sexual histories if one does not act upon or know how to adequately deal with the information obtained. Referral to GU medicine is always an option; however, much asymptomatic testing can be very easily promoted and undertaken in general practice and family planning clinics. A sexual history should be as routine as checking for diabetes or blood pressure and should certainly be mandatory as part of any routine contraception consultation.
Two-thirds of respondents were offering HIV testing in their clinic settings, 14% of them were not prior to attending the STIF course, one may conclude that it has been responsible for this increase in testing. However, 26% of respondents were still not offering HIV testing following the STIF course with 55% still not actively offering HIV testing to someone at risk of an STI. The STIF course includes a session on pretest discussion, which includes consideration of insurance and confidentiality (also included in the delegate manual). With some respondents siting confidentiality, lack of training, no perceived need and no demand should one ask – are we getting the right messages across? 4 HIV testing should no longer be accorded any special status and should be readily available. Lowering the threshold for HIV testing will lead to early diagnosis and treatment of infected individuals, which may prevent the development of AIDS and reduce ongoing HIV transmission. 5 As many respondents still refer to GU medicine, this suggests that there is much work to be done to engage general practice and contraceptive services in the role of basic STI screening. Until GPs feel that are adequately remunerated this may not change. Regarding the respondent who replied ‘difficult subject to broach in a contraceptive consultation’ one does wonder when else would be a better time to discuss sex and STIs!
Newcastle is a syphilis outbreak area with a 1000% increase in early infectious cases since 2002. This has been well-publicized at our STIF courses, especially in the years to come. It is therefore disappointing that only one-third of the respondents routinely offer syphilis serology, of these 37% did not before attending the STIF course. When GP data were reviewed, 65% who responded were not testing for syphilis if a patient was at risk of an STI; however, of the 32% who were testing, 61% had not tested before attending a course with 78% of these having attended a course during 2005 or 2006 when the outbreak was more publicized. It appears that the message of the syphilis outbreaks and increased prevalence of syphilis has been picked up by a few which may reflect more emphasis on this in the latter years.
When asked why they were not testing for syphilis many either referred on to GU medicine or refrained because of the perceived low prevalence. The respondent who replied ‘I have judged risk to be very low except in certain groups but I am aware I may not be identifying bisexual/homosexual or taking a full sexual history’ is honest and hopefully the questionnaire has stimulated a change in practice. As another respondent commented ‘don't immediately think of it each time but this questionnaire has reminded me.’ This shows that the initial STIF course has provoked interest and a change of behaviour in testing for syphilis in some, but that an update course may remind participants and give them the confidence to proceed with assessing syphilis risks and increased testing. The comments also suggest that the STIF course may need more specific teaching time spent on syphilis. However, fixed attitudes still exist as demonstrated by the respondent who does not routinely test for syphilis and stated ‘never seen any patients with positive serology in 25 years in practice’ – if you don't test then you won't identify any cases.
Ninety-six percent of respondents were offering chlamydia testing with 77% stating that they actively promote opportunistic testing to at-risk sexually active patients under the age of 25 according to the National Chlamydia Screening Programme (CSP). CSP was introduced in 2002 and only extended to full national coverage in 2007. There is less confidence in testing men for gonorrhoea. Eighty-four percent said that they offer testing, but of these 31% were confined to women only. Reasons stated for not testing were lack of availability of suitable swabs and refer to GU medicine. The STIF course does have a comprehensive session on swab-taking and these concerns should be dealt with on the course; hence these responses are disappointing.
Although the majority of participants (97%) felt that they were much more confident about dealing with STIs after the course there still appears to be reluctance to practice these ideas and skills on the shop floor, with many respondents failing to test for HIV, syphilis and gonorrhoea. If participants are still unsure about the importance of HIV and syphilis testing what hope have we for patients! We need to ensure a baseline of competence in sexual health for all doctors, not just those formally working as sexual healthcare providers. 6