
Abstract
In this structured review, we evaluated purulent vaginal and cervical discharge as diagnostic tests for pelvic inflammatory disease (PID). Using a pretest probability of PID (diagnosed clinically) of 50%, we used the odds-likelihood formulation of Bayes' theorem to calculate post-test probabilities of PID (proven by laparoscopy or endometrial biopsy). If abnormal discharge was present, the post-test probabilities of PID ranged from 50% to 73%, with a mean value of 57%. If abnormal discharge was absent, the post-test probabilities ranged from 24% to 52%, with a mean value of 39%. Therefore, the presence or absence of excess white blood cells in vaginal or cervical discharge was not particularly helpful in confirming or excluding PID in patients in whom the diagnosis was suspected from the clinical examination.
INTRODUCTION
As pelvic inflammatory disease (PID) is an infection that ascends from the cervix, it is reasonable to expect that cervical infection makes PID more likely. As indicators of the presence of PID, investigators have evaluated two clinical findings that may indicate cervical infection: the presence of excess white cells in vaginal discharge and of mucopus in the cervical os. 1–13
The presence of white blood cells (WBC) in vaginal discharge is not specific for cervical infection, because they can result from vaginitis as well as cervicitis. 14 However, experts have suggested that the presence and particularly the absence of white cells may be a helpful diagnostic sign. 8,12,14 This latter view seems to be supported by studies that have found high sensitivities for excess WBC as a diagnostic test for PID. In the five studies with the most favourable results, sensitivities have ranged from 0.80–0.89. 6,10–13 If the sensitivity is high, only a relatively small proportion of patients who have PID will have false-negative tests (no WBCs in the vaginal discharge), and it seems to follow that lack of WBC makes PID unlikely.
A favourable sensitivity may not mean that patients who have a negative test are unlikely to have disease. Sensitivity answers the question: What is the probability that a person with known disease will test positive? However, the clinician is usually more interested in the post-test probability of disease when the test is positive or negative. Post-test probability of a positive test answers the question: What is the probability that a person with a positive test actually has disease? The post-test probability of a negative test answers the question: What is the probability that a person with a negative test actually has disease? Post-test probabilities depend on the pretest probability of the disease and the sensitivity and specificity of the diagnostic test.
In this structured review, we evaluated the usefulness of excess vaginal and cervical WBCs as diagnostic tests for PID.
METHODS
Identification of appropriate studies
We performed a search using Ovid Medline and the search terms salpingitis OR adnexitis OR PID OR pelvic inflammatory disease AND diagnosis. We reviewed all possibly relevant articles among the 1028 found in the search. We also examined possibly pertinent articles and books in the bibliographies of the articles found in this search; and reviewed articles cited in the latest (fourth) edition of the textbook Sexually Transmitted Diseases. 14
Calculation of post-test probabilities
From the data available in the papers that we selected, we calculated two values: the probabilities that a patient has PID if she does or does not have excess leukocytes in vaginal or cervical discharge. The first of these values, the probability that a patient does have PID if there are excess leukocytes, is called the post-test probability of disease if the test is positive, and is the same as the predictive value of a positive test. The second value, the probability that a patient does have PID if there are no excess leukocytes in the discharge, is called the post-test probability of disease if the test is negative. It is equal to [1 − (predictive value of a negative test)], because the predictive value of a negative test is the post-test probability that a patient does not have disease if the test is negative.
For each study, we calculated the post-test probabilities of PID from the pretest probability of disease (the prevalence of PID in patients like the patient being tested) and the sensitivity and specificity of the diagnostic test, namely excess leukocytes in vaginal or cervical discharge. We calculated these probabilities using the odds-likelihood formulation of Bayes' theorem: 15
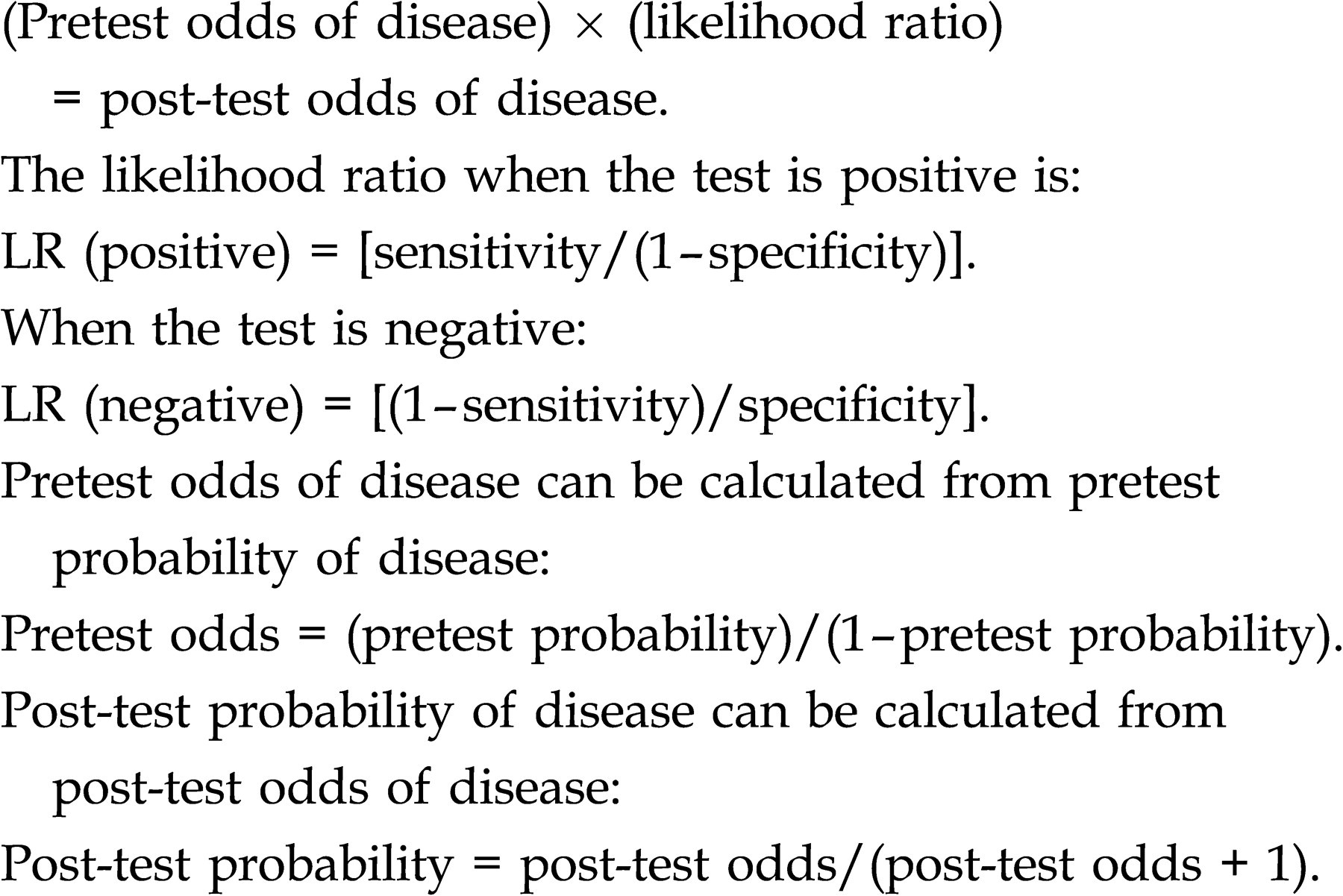
The pretest probability of disease is usually estimated. 15 We estimated the pretest probability for the presence of proven PID (proven by laparoscopy or endometrial biopsy) in patients who have clinical evidence of this disease (for example, lower abdominal and adnexal tenderness) to be 50 (50%). In other words, if PID is suspected on clinical grounds, we estimated that 50% of patients will actually have this disease. We believe that this value is reasonable based on the available literature: from 12 studies in which the clinical diagnosis of PID was confirmed by laparoscopy or by applying narrow clinical rules, Kahn et al. 16 found that 33–74% of patients suspected of having PID on clinical grounds actually had this disease. If we had chosen a larger pretest probability, the post-test probabilities, both positive and negative, would have been larger; if we had used a smaller pretest probability, the post-test probabilities would have been smaller.
Table 1 includes the calculated sensitivities, specificities and post-test probabilities of disease, and also the definitions of abnormal vaginal or cervical discharge for the articles that we included. As we mentioned above, the post-test probabilities were based on a pretest probability of 0.50.
Post-test probabilities of pelvic inflammatory disease (PID) in patients who did or did not have purulent vaginal and/or cervical discharge
*The post-test probabilities are based on a pretest probability of 0.50 (50%) (see text for definitions)
RESULTS
The post-test probabilities of proven PID if leukocytes were present in vaginal or cervical discharge ranged from 50% to 73%. The mean value with 95% confidence interval (CI) was 57%, 53–61% (Table 1). Therefore, given that the pretest probability was 50%, the presence of leukocytes did not increase the probability of PID enough to make this a particularly helpful test. Excluding Westrom's thesis 2,3 (whose results have not been reproduced elsewhere in the literature), the post-test probabilities of PID if leukocytes were absent ranged from 24% to 49%. The mean value with 95% CI was 39%, 35–42%. This mean probability is large enough that PID cannot be dismissed as a possible diagnosis, given its potentially severe long-term complications if it is not adequately treated.
Comments on the studies
Jacobson and Westrom's paper 1 is the classic evaluation of the diagnostic accuracy of clinical examination, using laparoscopy to confirm or refute the clinical diagnosis. Although they used ‘abnormal vaginal discharge’ as one of the several possible selection criteria to admit patients to the study, they also evaluated this for its diagnostic utility. What was meant by ‘abnormal’ discharge is not specified, but a subsequent report 4 suggested that this meant ‘purulent’ discharge. It is not clear if purulence was assessed visually or with a microscopic evaluation of the discharge. Because it was a selection criterion, in its evaluation as a diagnostic criterion the sensitivity was probably higher and the specificity lower than if purulent discharge was not a selection criteria: more subjects with or without proven PID would have had purulent discharge.
We were not able to obtain Westrom's thesis, 2 but he cites his thesis and gives summary comments on vaginal leukocytes as a diagnostic test in a chapter of the book on PID of which he is an editor. 3 He states that, in 327 women who had laparoscopically verified PID, ‘…leukocytes outnumbered all other cellular elements in the smear.’ In 105 women with presumptive PID who had negative laparoscopy, eight had normal smears. For these data, the sensitivity of excess vaginal leukocytes is 100% and the specificity is 8.2%. Because of the 100% sensitivity, lack of leukocytes rules out PID. However, this is the only report in which absence of leukocytes is very helpful diagnostically. It is not clear if leukorrhoea was a selection criterion for subjects, or whether these subjects were a subset of those in the study by Jacobson and Westrom. 1
Hagdu et al.'s 4 study evaluated a subset of those in Jacobson and Westrom, 1 namely those with an apparent first episode of PID; those with recurrences were eliminated. They also eliminated 76 women whose pelvic infections were apparently chronic, not acute. In this paper, ‘abnormal’ vaginal discharge is also called ‘purulent’ vaginal discharge. As was mentioned in the discussion of Jacobson and Westrom's study, 1 abnormal vaginal discharge was one of several selection criteria, probably affecting the values for sensitivity and specificity.
In the study by Simms et al. 5 the subjects include those evaluated by Jacobson and Westrom 1 and Hagdu et al. 4 Like Hagdu et al., they evaluated only first episodes of PID. They indicate that they included patients seen for an additional two years and have more patients with PID but fewer patients without PID, which is confusing.
Wolner-Hannsen et al.'s paper 6 again includes Westrom as a co-author and has a similar approach to the evaluation of PID as did Jacobson and Westrom. 1 However, this study only included woman with a positive culture for chlamydia and a negative culture for gonorrhoeae, and therefore represents a subset of women who are diagnosed with PID. Once again, purulent vaginal discharge was one of several possible selection criteria and was also evaluated as a diagnostic criterion. It was not made clear whether purulence was evaluated visually or with a microscope.
Tavelli and Judson undertook a different approach and therefore their results were not directly comparable to those in the other studies. They reviewed the records of their public sexually transmitted infection clinics and compared PID patients, diagnosed clinically (n = 114) to all patients who did not have PID (n = 8576). They did not verify PID with laparoscopy or endometrial biopsy; therefore they probably over-diagnosed PID, but their diagnostic approach is the one used by most clinicians. Among the diagnostic variables that they evaluated were purulent vaginal and purulent endocervical discharge; how the purulence was determined is not mentioned.
Both Rousseau et al. 8 and Bevan et al. 10 evaluated women who met clinical criteria for PID and confirmed the diagnosis with laparoscopy; Livengood et al. 9 used a similar approach on hospitalized women thought on clinical grounds to have severe PID. Rousseau et al. used abnormal vaginal discharge as one of the several selection criteria.
Peipert et al. 11 evaluated women who met clinical criteria for PID and confirmed the diagnosis with laparoscopy and/or endometrial biopsy. This paper also included information on patients who were at high risk for PID but did not meet the clinical criteria; we have considered only the first group in this report.
We found three studies that evaluated cervical mucopus as a diagnostic test for PID. Tavelli, in the study mentioned above, also assessed this variable. Peipert et al. 12 , in the first 58 patients enrolled in the PEACH study, which compared inpatient and outpatient therapy for PID, evaluated the combination variable of mucopus or leukorrhoea and used endometrial biopsy as the test to confirm PID. Their paper also includes data on a second group of patients in whom vaginal WBCs or cervical mucopus was one of the several selection criteria; they do not provide data to permit evaluation of post-test probabilities in this group. Peipert et al. 13 also reported on the complete PEACH study; for all but the first 58 subjects, leukorrhoea or mucopus was one of several possible selection criteria. Leukorrhoea was considered to be present if the number of polymorphonuclear WBCs was greater than the number of epithelial cells in at least four high-power microscope fields of vaginal discharge; cervical mucopus was present if yellow or green exudate was present on a swab used to obtain a specimen from the endocervix.
We have included the study by Yudin et al. 17 because it is widely cited. However, its subjects were not women who had clinical evidence of PID but instead were women at high risk for PID. Endometrial biopsy was used to confirm upper reproductive tract inflammation. Thus it is a study of silent endometritis.
DISCUSSION
Our review indicates that the presence of excess WBCs in vaginal or cervical discharge is not helpful in making a diagnosis of proven PID in patients in whom the diagnosis is suspected on the basis of the clinical examination, and their absence is not helpful in deciding that the patient does not have PID.
The available data have limitations. First, the reports do not have a consistent definition of excess WBCs in vaginal or cervical mucus. Secondly, in some studies, 1,4–6,8,13 excess vaginal WBCs and/or cervical mucopus were one of the several possible selection criteria for inclusion of subjects; this inappropriately increases the sensitivity and decreases the specificity of these diagnostic variables, compared with the values that would have been obtained if they had not been among the selection criteria. The specific effect of these alterations of the sensitivity and specificity on the post-test probabilities of disease is impossible to determine. Thirdly, several studies had relatively few subjects (Table 1), and so the CIs around the sensitivities and specificities, and therefore around the post-test probabilities derived from them are wide.
Fourth, the selection criteria for subjects (the clinical diagnostic criteria for PID) often differed among the studies. Finally, laparoscopy and endometrial biopsy are not 100% accurate in confirming the diagnosis of PID; false-negative and false-positive findings can occur, and it is not clear that the presence of endometritis necessarily indicates the presence of salpingitis, a pathological condition that causes most of the long-term complications of PID. 14 However, since all research has similar findings, our conclusion about the lack of utility of these diagnostic tests seems appropriate.
The latest edition of the textbook, Sexually Transmitted Diseases, 14 states that ‘If pelvic examination findings suggest PID in a patient with a negative pregnancy test, the presence of MPC [mucopurulent cervicitis] or an increased number of WBCs on a wet mount of vaginal fluid (e.g. number of WBCs exceeds number of epithelial cells) suggests PID… However, PID is unlikely if… the wet mount shows normal lactobacilli and no WBCs.’ The data presented in our study do not support the assertions concerning the usefulness of the presence or absence of vaginal WBCs as in the diagnosis of PID.