
Abstract
HIV patients frequently have opportunistic oesophageal infections. We report Haemophilus ducreyi genetic material detected by polymerase chain reaction in biopsies of oesophageal lesions in three HIV-1-infected patients. This finding may be an indication of its aetiopathological role in oesophageal lesions of HIV patients.
INTRODUCTION
AIDS encompasses several clinical manifestations, ranging from asymptomatic infection to development of severe and potentially lethal opportunistic infections. Oesophageal disease occurs in as many as 40% HIV patients at some point of the HIV infection, 1 infection being the most important aetiology. Candida albicans is the most prevalent infection, followed by cytomegalovirus and herpes virus infections. 2,3 Other unusual agents have also been implicated in the aetiology of oesophageal disease.
A considerable part of oesophageal lesions does not have an identified agent, and are considered idiopathic. 2,4 These idiopathic oesophageal lesions can be due to HIV infection, apoptosis or another agent not yet identified by traditional diagnostic methods. 5,6 Considering the efficacy of currently available treatment for most of the pathogens, a definitive diagnosis has an important prognostic implication. Therefore, the use of novel diagnostic methods should be considered in these patients.
Owing to the diverse sexual activity described by our patients, we hypothesized that Haemophilus ducreyi could have an aetiopathologic role in oesophageal lesions of HIV-1-infected patients, and polymerase chain reaction (PCR) could improve its detection. Therefore, we studied the role of PCR to detect H. ducreyi in biopsies obtained from oesophageal lesions of HIV-1-infected patients.
METHODS
Seventy-nine HIV-1-infected patients presenting with gastrointestinal symptoms and who were attended at the Clinical Hospital of the University of São Paulo Medical School at Ribeirão Preto were included in the study. Seventy patients were submitted to one upper endoscopy, eight patients to two upper endoscopies and one patient to three upper endoscopies, with a total of 89 procedures. Ninety-six oesophageal biopsies were collected, kept either in liquid nitrogen or at −70°C, and processed for PCR amplification. The clinical characteristics of these HIV-1-infected patients are listed in Table 1. Biopsies were also sent to routine histopathological studies according to our hospital protocol. The need for a biopsy was defined by the medical team, without any interference by the authors. The study was approved by the local Ethics Committee.
Characteristics of HIV-1-infected patients
*These results are expressed in mean and limits
†Twenty patients had more than one primary symptom
All biopsies were thawed at room temperature in a laminar flow cabinet and grounded with a sterile scalpel. The material was transferred to a sterile tube, and tissue lysis was performed by adding 500 μL of lysis solution (10 mmol/L Tris-HCl, pH 8.0; 10 mmol/L EDTA, pH 8.0; 100 mmol/L NaCl; 1% SDS) and 1 μL of proteinase K (20 μg/mL), followed by incubation at 55°C for two hours. The DNA extraction was carried out by adding 500 μL of phenol equilibrated with TE buffer (10 mmol/L Tris-HCl, pH 8.0; 1 mmol/L EDTA). The mix was agitated and centrifuged at 13,000
We used specific primers to H. ducreyi, designed to amplify the 16S rRNA gene. 7 The amplicon for H. ducreyi has an expected size of 799 base pairs. In all reactions, negative and positive controls were added. As a positive control, extracted DNA from a reference strain of H. ducreyi obtained from Adolfo Lutz Institute, São Paulo was used in all PCR reactions.
RESULTS
The PCR was performed in all oesophageal biopsies. In three biopsies from three different patients, the PCR for H. ducreyi was positive (Figure 1). The characteristics of these HIV-1-infected patients with a positive PCR for H. ducreyi, and the endoscopic and histopathological findings are given in Table 2. Only one of these patients, patient 3, had a history of a sexually transmitted disease, i.e. syphilis. Patient 2 had a history of drug abuse and patient 1 reported unprotected sexual intercourse. The PCR was repeated with the same biopsies and the positive result for H. ducreyi was confirmed. Because these biopsies were retrospectively analysed, it was not possible to ascertain whether these patients were treated or not for H. ducreyi infection, and they were no longer available for medical evaluation.
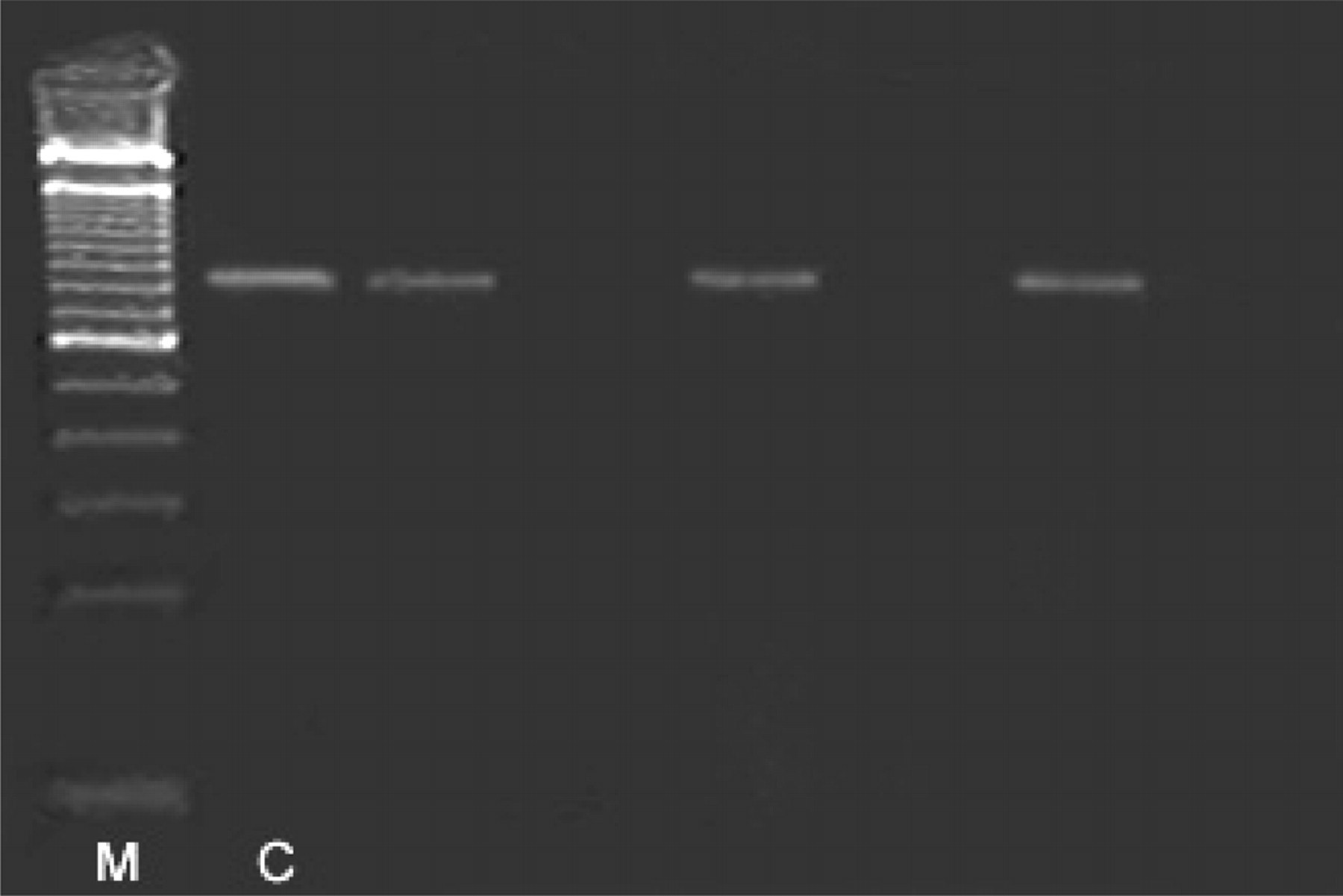
Detection of H. ducreyi genome on 1% agarose gel electrophoresis, stained with ethidium bromide. From left to right: molecular weight marker (M) (100 pb DNA ladder), positive control (C) and three biopsies positive to H. ducreyi. The amplicon for H. ducreyi has 799 base pairs. As a positive control, extracted DNA from a reference strain of H. ducreyi obtained from Adolfo Lutz Institute, São Paulo was used
Characteristics of HIV-1-infected patients with oesophageal lesions whose polymerase chain reactions were positive to H. ducreyi
DISCUSSION
This study is the first to demonstrate the presence of H. ducreyi genetic material in oesophageal biopsies of HIV-1-infected patients. This finding raises the need for a better understanding of the aetiology of oesophageal lesions in HIV patients, especially in patients with a severe immunodeficiency.
Owing to the diverse sexual activity described by our patients and considering the different modes of acquiring sexually transmitted diseases, the rationale of this study was to evaluate the role of sexually transmitted infections in oesophageal ulcers of HIV patients. Therefore, we also performed PCR with respect to syphilis in all samples, but the results were all negative.
The H. ducreyi genetic material was detected by PCR in three of the 79 patients studied. Two of these patients had a severe immunodeficiency, demonstrated by a CD4+ T-cell count of <100 cells/μL. This finding has been indicated as a risk factor for the development of oesophageal lesions by atypical pathogens. 1
H. ducreyi is a strict human pathogen, and there is no known animal or environmental reservoir. Human-to-human transmission of H. ducreyi is primarily by sexual means alone. 8 The route of infection of the patients in our study is unclear since it was not possible to obtain this information either from the charts, due to the retrospective design of the study, or in person, due to the death of these patients.
Chancroid has a worldwide distribution, typically associated with low socioeconomic status and precarious hygiene. It is a common cause of genital ulcers in developing countries, predominantly in men with a history of promiscuity. 9 The prevalence of chancroid in Brazil is not known. Non-genital chancroid, such as of the mouth, fingers, thighs, abdomen, feet and limbs, is rarely described. 10,11 Oesophageal lesions caused by H. ducreyi have not been previously reported.
The diagnosis of H. ducreyi based on morphology by direct microscopy, with the finding of Gram-negative cocobacilli, has a low accuracy (30–50%). 12–14 The culture was considered the ‘gold standard’, but is a difficult method, requires special cultural media and has a sensitivity of only about 75% at best. 15–17 In an attempt to improve the sensitivity of the diagnosis, DNA amplification techniques have been developed. 18 According to Chui et al., 7 the PCR used in this study has a sensitivity of 83–98% and a specificity of 51–67%. 7 The low specificity of PCR in some studies probably reflects the poor sensitivity of culture for diagnosing chancroid.
In all three patients, the histopathological evaluation demonstrated another agent (candida, mycobacterium and herpes virus) that could be the aetiology of the oesophageal lesions. However, we believe that the finding of another pathogen in these patients does not rule out the aetiopathological role of the H. ducreyi, since several simultaneous pathogens have been described in HIV patients with oesophageal symptoms. In the majority of patients, candida is one of the co-infectious agents. 1,2
The finding of H. ducreyi genetic material in oesophageal lesions of HIV patients raises the possibility of a new cause of oesophageal lesions and creates the necessity for further studies for a better understanding of its role in oesophageal ulcer causation in HIV patients. Epidemiological studies should be undertaken to determine the likely mode of transmission and reservoir for H. ducreyi.
In conclusion, the finding of H. ducreyi genetic material in oesophageal lesions is an indication that a new pathogen may be playing a role in the causation of gastrointestinal lesions of HIV patients, and clinicians involved in the care of HIV-infected patients should consider H. ducreyi in the aetiology of oesophageal ulcers.