
Abstract
Summary
We introduced a Nurse/Health Advisor-led fast-track service for treating patients diagnosed with chlamydia outside a genitourinary medicine setting and contacts of chlamydia/non-specific urethritis/cervicitis wherever diagnosed. Asymptomatic patients were treated without initial testing and asked to return for full screening at four to six weeks. We assessed the efficacy and safety of the system and need for follow-up after treatment. Case-notes of 226 patients (121 men and 105 women) were analysed, of whom 140 attended follow-up. With the exception of one case of gonorrhoea, no other serious sexually transmitted infection was detected. Twenty-seven (19.2%) patients were re-treated for either chlamydia (six patients, 4.4%) or non-specific genital infection or because of having unprotected intercourse with untreated or partially treated partners. We conclude that in our relatively low-risk population, our fast-track service is safe and effective. Test of cure for chlamydia seems essential because of the high percentage of patients requiring re-treatment.
INTRODUCTION
In 1999, we introduced a Health Advisor-led fast-track system (FTS) to treat patients with Chlamydia trachomatis infection that had been diagnosed in our hospital's colposcopy unit. 1
An audit showed that the fast-track care pathway was efficient and we decided to extend the service to include patients with proven chlamydia infection referred from family planning clinics, local general practitioners, our obstetrics and gynaecology department and other health-care settings. In October 2005, the fast-track service was further extended to include all heterosexual patients who were contacts of proven chlamydia, non-specific urethritis and non-specific cervicitis wherever diagnosed. This was introduced so that these patients could be seen and treated quickly. In 2007 we decided to assess the safety and efficacy of the extended treatment system.
In addition, because high rates (13.3–18%) of persistent chlamydia infection following treatment had been reported in various studies, we were also interested in assessing our rates of persistent chlamydia infection after fast-track treatment. 2,3 For this study we selected only those patients seen within the FTS who had tested positive for C. trachomatis or were contacts of proven chlamydial infection.
PATIENTS AND METHODS
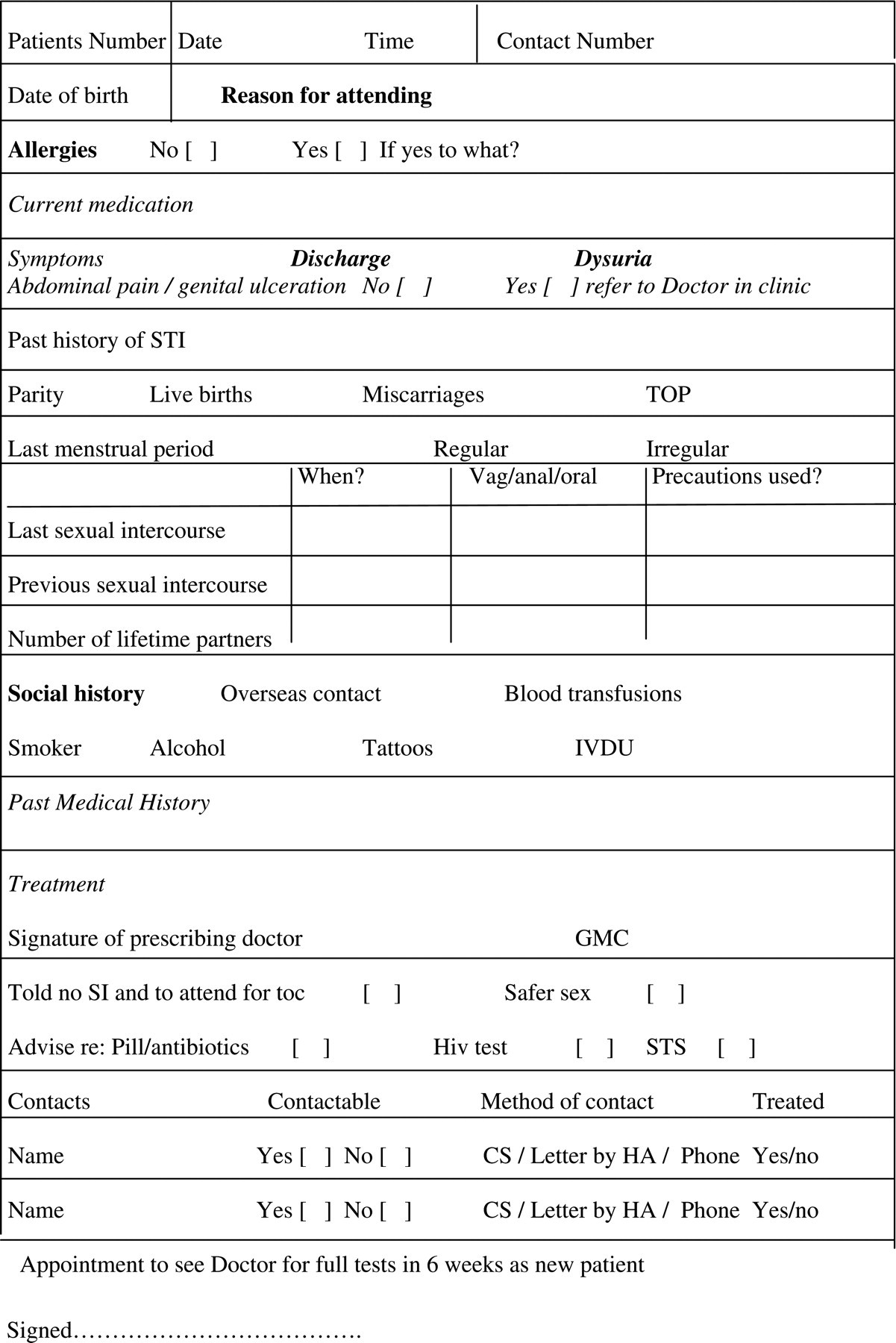
In the FTS, patients were seen by a health advisor or a nurse who completed a simple proforma (Figure 1). Blood tests for syphilis and HIV were offered and necessary treatment and partner notification arranged. Symptomatic patients were referred to a clinic doctor for full evaluation during their initial visit to exclude complicated chlamydial infection or other serious pathologies. All patients were given an appointment to be seen at four to six weeks for full screening.
Management of female contacts of male chlamydia-positive patients
We did a retrospective study analysing the case-notes of all patients who were treated by the fast-track service between October 2005 and February 2007. For our study we then selected only those patients who had proven chlamydial infection or were proven chlamydia contacts, so that we could assess chlamydia detection rates after therapy.
The following data were collected: patients age and gender, previous history of sexually transmitted infection (STI), symptoms at their initial visit, where patients were diagnosed, time interval for patients or partners to be seen in GU medicine, number of patients who had blood tests for HIV and syphilis during their initial visit, the number of patients attending at four to six weeks for full tests, other infections that were identified during full assessment, number of patients tested positive for C. trachomatis after treatment and number of patients requiring re-treatment for any reason. To assess the disruption to routine clinics we also looked at the number of patients who had to see the doctor during the first visit. Details of treatment during first visit and re-treatment details were also noted.
RESULTS
During the study period, 445 patients were treated by the FTS. Of these, 249 patients fitted our selection criteria, and 23 notes were not available. The final study group of 226 patients were all heterosexual and comprised 105 women and 121 men.
Age group distribution is shown in Table 1.
Age group distribution of patients
Of the 226 patients, 40 (17.6%) had a previous history of STI, of whom 22 had had chlamydia. Of the 121 men, 101 (83.5%) and 69 (65.5%) of 105 women were asymptomatic. Of the 226 patients, 18 (8%) were seen by a doctor and five of these merited full screening during their initial visit. One of the five patients had testicular pain and one had an epididymal cyst. Among the three women who had full tests, one was a pregnant woman who was a contact of gonorrhoea and chlamydia and two had abdominal pain needing assessment for possible pelvic infection. Twenty-five (11%) patients had blood tests for syphilis and HIV during their first visit.
Ninety (39.8%) patients were contacts of index patients diagnosed with chlamydia in the GU medicine clinic. Twenty-six (11.5%) patients were referred from our colposcopy unit and a further 47 (20.8%) patients/contacts were referred from other units within the Department of Obstetrics and Gynaecology. Ten other patients/contacts were from family planning clinics and 25 (11%) from local general practitioners. The remaining 28 (12.4%) patients were contacts of patients diagnosed with chlamydia elsewhere.
One hundred and twenty-six (55.6%) patients were seen within four weeks of their diagnosis or their partner's diagnosis. Twenty-five were seen within two months and four were seen after two months. The time interval was not known for the remaining 65 patients. None of the delays were related to inability to access GU services since all were offered same day appointments.
Of the 226 patients 140 (62%) (74 women and 66 men), attended follow-up for full tests. Of these, a record of compliance was noted in 138 patients (98.6%) notes. Among the 138 patients, one had missed four doxycycline capsules giving a recorded compliance of 99%.
There was no record of abstinence in eight of the 140 notes but of the remaining 132 patients, 71 (53.7%) said they had abstained from sex from the time they were treated. Thirteen of the returnees had had unprotected sexual intercourse with an untreated or partially treated partner and were re-treated. Of these, four did not attend follow-up for full tests after re-treatment.
The remaining 136 patients had full tests and six of them (4.4%), three men and three women were positive for chlamydia. Five of the six treatment failures had been treated with doxycycline 100 mg twice daily for seven days and one was treated with azithromycin 1 g. One man who had been treated as a chlamydia contact had positive chlamydia swabs twice on tests of cure, which were taken more than six weeks apart after initial and re-treatment. All six patients with treatment failure said they had been abstinent but one had missed four doxycycline capsules. One woman had gonorrhoea, which was probably a new infection (she had recurrent chlamydia at her gonorrhoea test of cure [TOC]), six of the 136 patients had non-specific urethritis, two had non-specific cervicitis, eight were noted to have genital warts, one had lichen sclerosis and one had a urinary tract infection. Nine patients were treated for bacterial vaginosis and 17 were treated for genital candidiasis. There were no cases of HIV or syphilis. Excluding patients re-treated because of unprotected sex, and when all infections are included, 43 of the 136 (32%) required some form of further treatment.
Overall, 27 (19.2%) of the 140 patients required re-treatment for chlamydia/NSU/NSC or unprotected sex with untreated partner.
One hundred and forty-nine patients were treated with doxycycline 100 mg twice daily for seven days and 59 had azithromycin 1 g as a single dose. Eighteen women with risk of pregnancy and/or pregnant women were treated with erythromycin 500 mg four times a day for 10 days and one, who was unable to tolerate erythromycin, was given amoxicillin 500 mg three times a day for one week.
DISCUSSION
The rise in STIs has increased the workload and waiting times for GU medicine services and led to a variety of innovative ways of screening and service delivery. These include community-based nurse-led sexual health clinics, screening and treatment of STIs in family planning clinics, chlamydia screening programme and commercial tests such as Boots Chlamydia tests. 4–6
Before we had our fast-track service many contacts of chlamydia had to wait to be seen and anecdotally we noted that some visited their GP where often no tests would be carried out and sometimes inappropriate treatment given. Our FTS allowed patients found to have chlamydia outside our GU medicine clinic and all chlamydia contacts wherever diagnosed to have immediate access to treatment. Our study has shown that the FTS appears to be a rapid, safe and effective way of treating such patients.
Our FTS is safe in that all patients who had symptoms suggestive of complicated genital tract infection were referred immediately to a clinic doctor. There was minimum disruption to routine clinic since only a small proportion (8%) of these patients needed to see the doctor and only 2% required full screening.
There were no serious infections identified during full screening after treatment in our cohort of patients apart from one patient who had gonorrhoea, which was almost certainly a new infection. This is reassuring since it is likely that a similar or possibly even lower rate of genital tract infection would be present in the 38% of patients who did not reattend for full tests. The main issue highlighted in the study was the fact that only 25 patients (11%) had blood tests during their first visit. More emphasis is now placed on taking blood tests during the initial visit but given that the FTS is only used for our heterosexual patients and that in our local population the incidence of syphilis and HIV in this group is very low, it is unlikely that any cases were missed.
Effective partner treatment strategies play an important role in preventing reinfection and spread to others. Recently, a study assessing the effect of expedited partner treatment was carried out by Golden et al. who randomly assigned heterosexual patients with gonorrhoea or chlamydial infection into two groups. 7 One group had expedited treatment for their partners (i.e. treatment given to the index patient to give to their partner) and the other had standard referral for their contacts. The incidence of persistent infection was then assessed in the patients from both groups. Results showed that providing treatment for sexual partners without prior medical evaluation significantly reduced persistent infection and the incidence of patients having sex with an untreated partner. With the high workload and long waiting lists in many GU clinics our FTS system appears to be effective with the added benefits of ensuring compliance, providing TOC and screening for other infections in this high-risk group.
BASHH guidelines state that TOC for uncomplicated chlamydia is not indicated but management of chlamydial infections varies in different clinics and TOC continues to be offered in some GU medicine departments. 8–10 In the recent study by Golden et al., persistent chlamydia infection was noted in 8% of women after treatment and the authors felt it may represent treatment failure rather than reinfection. 4 Horner has also suggested the possibility of heterotrophic resistance in patients with high chlamydia load and emphasized the urgency of further treatment studies, especially in women. 11 The role of antimicrobial resistance in chlamydia treatment failure is unclear but persistent/recurrent infection can be unacceptably high as shown in multicentered cohort study by Whittington et al. 12,13 This study of 1194 women with chlamydia revealed a 13.4% rate of persistent infection/reinfection after a median of 4.3 months. 14 The authors suggested that strategies for treatment of male partners should be developed and that women should be re-tested after a few months. In our study, TOC for C. trachomatis was positive in 4.4% of patients tested and in all, 19.2% of patients required re-treatment for either proven chlamydia or possible chlamydial infection. Taking into account a recent paper which showed nucleic acid amplification test (NAAT) positive patients may actually have low transmissibility; our study cohort may have included many contacts who may not have been initially chlamydia-positive. 15 This would make the incidence of our positive tests after treatment even more significant. Our results supports continued TOC's for chlamydia since otherwise significant numbers of patients may be at risk of serious complications and add to the infection pool.
Furthermore, emotional issues concerning TOC for chlamydia has been investigated in a recent study by Piercy who interviewed 50 heterosexual patients who had chlamydial infection. 16 Piercy concluded that ‘the retest occupied a pivotal position in the infection experience and was invested with symbolic significance because it provided a means by which to deal with feelings of bodily pollution’. The TOC was considered to be a right of passage into wellness and Piercy suggested that if re-testing is not offered patients may use opportunistic chlamydia screening inappropriately with consequent cost and resource implications. Women especially are more anxious in view of implications for future fertility. 17 In our population TOC seems to be essential as it shows an unacceptably high level of persistent infection. It is also likely that our patients benefit psychologically from confirmation that the infection has gone. We feel chlamydia FTS ensures that appropriate patients are seen quickly and treated for chlamydia. One test for chlamydia carried out six weeks after treatment reassures the patient and excludes persistent infection.
One concern we have is that we may now be treating chlamydial infection too quickly. SAFF targets for 48-h access have been vigorously implemented in our area on the grounds that rapidly treating STIs, in particular, chlamydia is good for our populations' sexual health. However, a recent paper by Rekart and Brunham intriguingly moots that if ‘we treat Chlamydia early we reduce the body's ability to fully respond immunologically and this increases the likelihood of reinfection upon re-exposure’. 18 They suggest that the development of an antichlamydial vaccine may be the best long-term objective. At present, we follow national guidelines and treat patients as soon as possible but feel that further research is needed to reassure us that rapid treatment programmes are not harming patients in the long term.
CONCLUSIONS
We conclude that if we accept the paradigm that rapid treatment of chlamydial infection is beneficial to patients, then our FTS of assessing and treating chlamydia-positive patients and their contacts appears to be rapid, safe and effective. Also, contrary to BASHH guidelines, it appears that TOC for uncomplicated genital chlamydial infection is of value and we feel that larger studies are urgently needed to see if current guidelines need to be reassessed.