
Abstract
Aspergillus infections are rare opportunistic infections in the course of AIDS and they mostly present as invasive pulmonary disease. Owing to the prolonged survival of profoundly immunocompromised patients with AIDS, invasive pulmonary aspergillosis is being reported with increased frequency. However, although pulmonary aspergilloma has been well described in immunocompetent patients, it has been rarely reported in AIDS patients. The treatment for pulmonary aspergilloma remains challenging and often needs lifelong treatment to minimize fatal haemoptysis, which can occur in up to 25%, and progression to secondary invasive aspergillosis. We report a case of pulmonary aspergilloma in a severely immunocompromised patient with AIDS who stopped taking systemic antifungal treatment in April 1998 and remained well with little progression of invasive aspergillosis up until March 2002 when he died of acute pancreatitis related to a drug interaction of didanosine and tenofovir.
CASE REPORT
A 50-year-old Caucasian married heterosexual presented with cavitating left apical pulmonary tuberculosis in May 1995 and was subsequently found to be HIV antibody positive. He was successfully treated with antituberculous therapy (Figure 1). He was commenced on antiretroviral therapy (ART) (zidovudine and didanosine) and co-trimoxazole, as his CD4 count was 130 cells/mm3 and remained well until April 1997 when he developed fever, cough, night sweats and weight loss. Chest radiograph showed infiltrates in the previous left apical cavity (Figure 2). The CD4 count was 70 cells/mm3 and neutrophil count was 2.3 × 109/L. Sputum investigations, bronchoscopy and larvage did not reveal any evidence of tuberculosis or fungal infections. His antiretroviral regimen was changed to stavudine and lamivudine but he declined a protease inhibitor. Sputum testing revealed Aspergillus fumigatus six months after his initial symptoms. The chest radiograph showed evidence of aspergilloma (Figure 3) and aspergillus precipitin was detected in the blood. He was initially treated with amphotericin followed by oral itraconazole 400 mg daily. The patient stopped taking oral itraconazole of his own accord after four months.
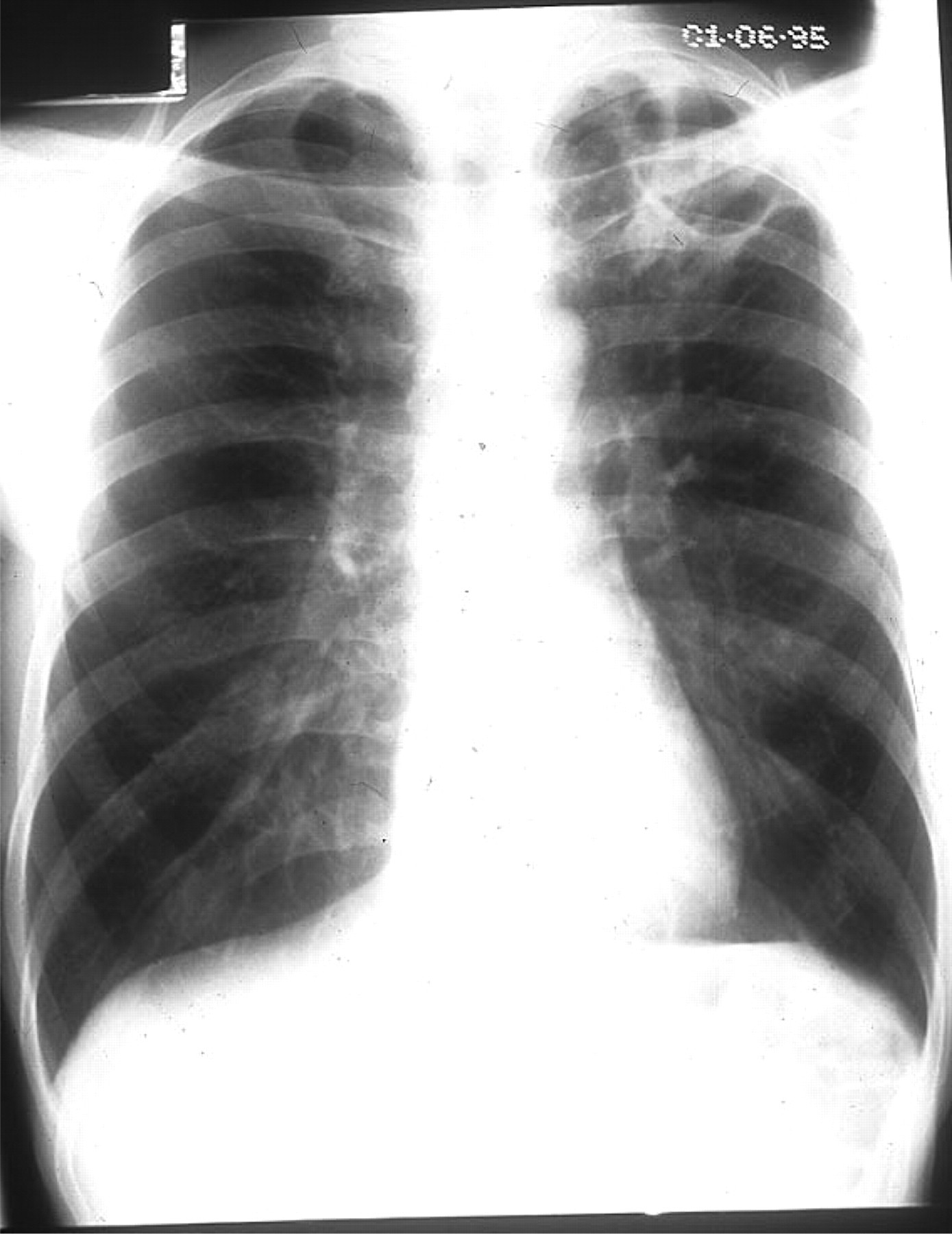
Left apical thin-walled cavity from previous tuberculosis in June 1995
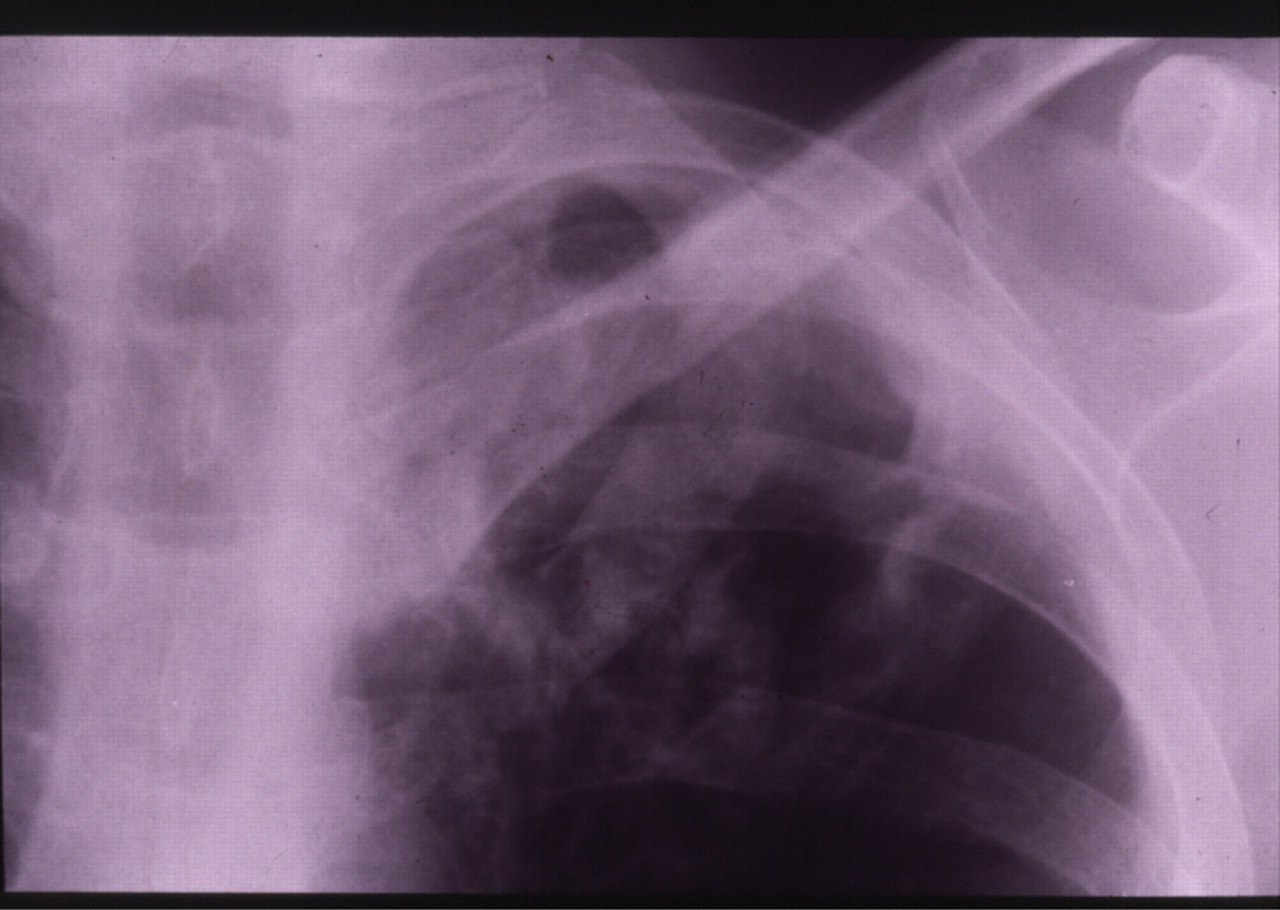
Infiltrates in the cavity
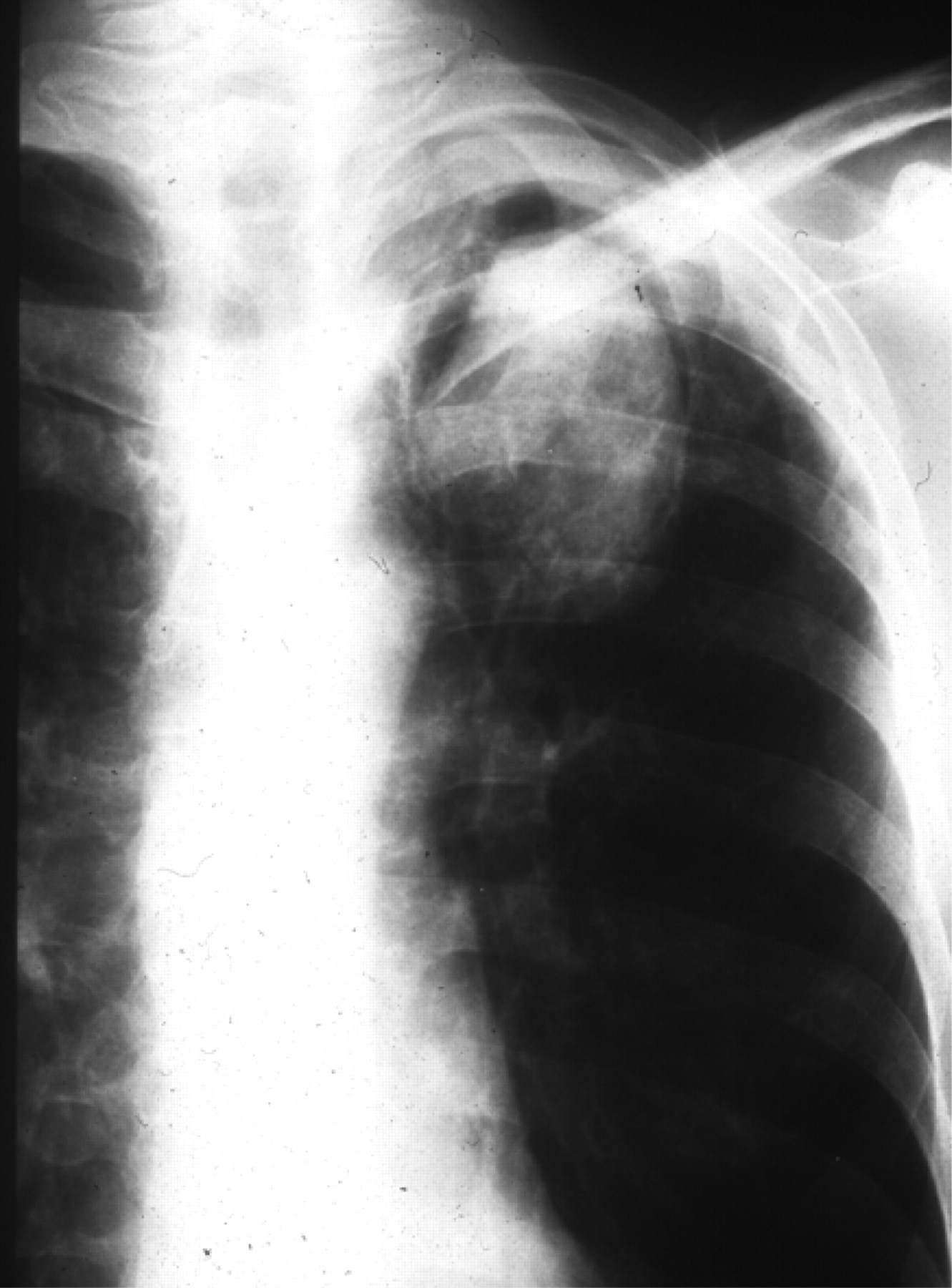
Aspergilloma with halo of air around the lesion in October 2001
Unfortunately in March 2000, he developed cytomegalovirus retinitis in his right eye when his CD4 count was 30 cell/mm3. This was successfully treated with cidofovir infusion.
After a genotype resistance test, the antiretroviral regimen was changed to stavudine, didanosine and lopinavir/ritonavir combination in November 2000. The HIV RNA level dropped from 240,000 copies/mL to zero, but his CD4 count remained low at 64 cells/mm3. A chest radiograph in May and October 2001 showed no significant change. In 2001 complete viral suppression was achieved, but in November 2001 the patient stopped all his medications feeling increasingly unwell and attributing his symptoms to the boosted lopinavir. In December 2001, the combination of stavudine, didanosine (250 mg) and tenofovir was commenced.
In January 2002, his viral load was 194 × 103 copies/mL and CD4 was 20, all other biochemical parameters including amylase were normal at this time.
In February 2002, he was admitted with nausea, vomiting and abdominal pain and his admission serum amylase was 3972 U/L. A diagnosis of iatrogenic acute pancreatitis was made and all ART was stopped. He was managed conservatively. Despite normalization of his amylase levels, he succumbed to adult respiratory distress syndrome (ARDS) in March 2002 (Figure 4). 1

Adult respiratory distress syndrome
DISCUSSION
Invasive pulmonary aspergillosis has been frequently described in patients with leukaemia and bone marrow and heart transplant recipients. 2,3 However, in patients with AIDS, aspergillosis infections are rare. Neutropaenia and corticosteroid use are well-established risk factors for the development of aspergillosis, but our patient had neither of these risk factors. 4
The incidence of pulmonary aspergilloma may increase with the rise in the incidence of pulmonary tuberculosis and other causes of cavitatory lung diseases such as Pneumocystis jirovecii pneumonia, bacterial lung abscesses and Kaposi's sarcoma in AIDS patients. 5 Early diagnosis is crucial in the management so that early treatment, which is usually lifelong, may prevent the incidence of invasive pulmonary aspergillosis and fatal haemoptysis in AIDS patients. 6–8 Surgical resection carries a significant mortality in immunocompromised HIV-positive patients. 9 Despite stopping suppressive itraconazole therapy for four years, a pulmonary aspergilloma did not significantly progress and may indicate that long-term suppressive antifungal therapy is not always needed, even when a patient remains severely immunocompromised, as in our case. Our patient died of ARDS due to acute pancreatitis, which is a well-recognized complication of didanosine and tenofovir increases systemic exposure of didanosine. 10
Footnotes
ACKNOWLEDGEMENT
The author would like to thank Dr A Blackwell for her assistance with the manuscript.