
Abstract
Gonococcal isolates from genitourinary (GU) medicine clinic attendees in Glasgow, Scotland were typed using Neisseria gonorrhoeae multiantigen sequence typing (NG-MAST). Correlation between named partners (contacts) and NG-MAST type was sought and associations between specific NG-MAST types, and the social, epidemiological and geographical data were explored. We found NG-MAST typing to be a supportive and confirmatory tool for contact tracing. Specific NG-MAST types were found to be associated with distinct characteristics such as sexuality or chlamydial co-infection. An increased number of gonococcal infections were reported from those resident in deprived areas of Glasgow than from those resident in more affluent areas. However, there was no clear geographic clustering of specific NG-MAST types found within the city. Routinely observing the spread of common strains of gonorrhoea is likely best done from a larger geographical perspective unless a specific outbreak occurs.
INTRODUCTION
Gonorrhoea is the second most common bacterial sexually transmitted infection in the UK and has a complex epidemiology. Strains of Neisseria gonorrhoeae can be differentiated and characterized by different methods. Traditionally antibiotic susceptibilities and phenotypic methods have been used. Molecular-based methods, which provide a higher degree of discrimination, include opa-typing 1 and N. gonorrhoeae multiantigen sequence typing (NG-MAST). 2 Opa-typing has been used to analyse sexual networks 3,4 but is laborious on large numbers of isolates and the results between laboratories cannot be easily compared. The NG-MAST method detects variation in the Por and Tbpb genes, and the online internationally accessible NG-MAST database 5 allows each isolate to be assigned a numeric sequence type (ST). NG-MAST is highly discriminatory, convenient and non-subjective, allowing local, national and international comparison of data.
In Glasgow, the largest city in Scotland, the annual incidence of gonococcal infection increased by 250% between 1994 and 2000. 6 A knowledge and understanding of the microepidemiology of gonorrhoea is one component that can help develop effective public health measures and previous work has shown clear geographical demographic demarcation of specific NG-MAST types within Scotland. 7
In this study, we investigated all GU medicine clinic attendees in Glasgow who were diagnosed with gonorrhoea during a 12-month period in 2003–2004 and combined NG-MAST data with clinical and demographic data. We sought correlation between partner (contact) clinical data and typing data, and evidence of geographical social or epidemiological distribution of clusters of gonoccocal infection within Glasgow itself.
METHODS
Participants
All adults (16 years and older) who attended Glasgow's main genitourinary (GU) medicine clinic and in whom N. gonorrhoeae was isolated during the study period 27 February 2003 to 8 January 2004 were eligible for the study (see Figure 1).

Flowchart showing participants and the origins of data used
Data collection
Demographic characteristics and key health-care outcomes were extracted from laboratory and clinical records for all participants. Additional information on sexual contacts during the last three months was obtained from routine case-note histories and contact tracing. Residential postcodes were classified using the Carstairs deprivation classification. 8
To broadly detect for possible geographic clustering of strains, the cases who were resident in Glasgow were additionally identified by their area of residence within the city, north, south, east or west.
Participants were invited to self-complete a questionnaire, eliciting detailed demographic, social and behavioural information, including circumstances surrounding participants' three most recent sexual ‘partnerships’ (of any duration). Informed consent was obtained by a research nurse.
Molecular typing of N. gonorrhoeae
Isolates from each episode of gonococcal infection during the study period were retrospectively typed using NG-MAST as originally described 2 with minor alterations to the method. 9 Each gonococcal isolate was assigned an ST. Where the Por or TbpB allele or the combination of alleles was not previously known, a new ST was assigned.
The study was approved by the local NHS Ethics Committee.
RESULTS
A total of 178 individuals diagnosed with gonorrhoea during the study period were eligible for inclusion. Of these, 170 were sequence-typed and each ST was matched to its case with full demographic and clinical outcome data. One isolate was non-viable; seven isolates were not available for the study.
Of the 170 isolates typed, 65 completed the detailed questionnaire about social and sexual networks.
NG-MAST types
Overall there were 69 different genotypes comprising 37 single isolates, 14 pairs and 18 clusters of between 3 and 13 isolates. Eighteen isolates were assigned new STs.
Using the extra data obtained from the self-completed questionnaires and linking it with the corresponding STs gave no link between ST and employment status, income group, school-leaving age, qualifications obtained, recreational drug taking or travel with work.
The majority of isolates (129; 75.9%) were from individuals resident in Glasgow and were represented by 58 different STs. Among 60 men who have sex with men (MSM) 28 different STs were found. Among 110 heterosexual men and women 51 STs were found. Demographic data for those patients represented by the 10 most frequent ST isolates are shown in Table 1. Some STs were associated with a particular demographic characteristic (e.g. age-range or sexuality, see Figure 2).
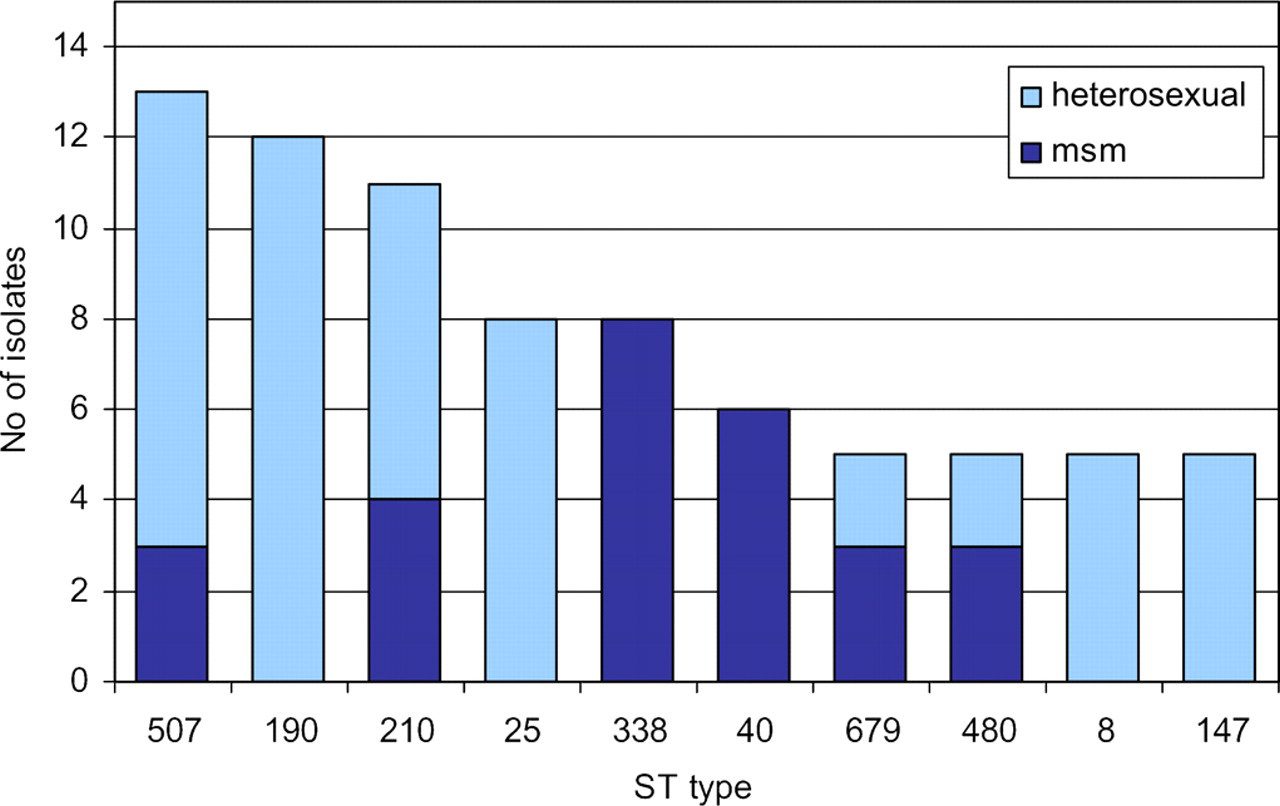
Top 10 sequence types (ST) split by sexuality. MSM = men who have sex with men
Characteristics of the 10 most common NG-MAST clusters
NG-MAST = Neisseria gonorrhoeae multiantigen sequence typing; MSM = men who have sex with men
Contact concordance
Twelve pairs of individuals who mutually named each other had gonococcal isolates with concordant STs. For these individuals, each reported between one and three sexual contacts in the preceding three months; however, a maximum of only one contact per index case was recorded as being identified and treated.
There were four pairs of named contacts where one strain in each pair was not typed (due to being outwith the study criteria). One heterosexual pair was infected with completely different strains having differences in both Por and Tbpb alleles. Both strains had identical antibiotic sensitivities. Only one of the pair was symptomatic and only one sexual partner was reported by each in the preceding six months, although one had recently been a commercial sex worker.
Co-infection
Overall chlamydial co-infection rate was 28.7% (49/171). There was significant variation between the types and co-infection rate. MAST types 8 and 25 had a high percentage of chlamydial co-infection (80% and 62.5%, respectively) and both were characterized by mainly heterosexual and under 25 years age group.
New NG-MAST types
There were 18 STs that had not previously been reported at the time of the study, accounting for 24 isolates. The majority of these were single isolates (13), four were pairs and one cluster of three isolates. One of the pairs had mutually named contacts. Five of the new STs were associated with anonymous sex (sex with a previously unknown partner met exclusively and intentionally for sex) and/or travel abroad or outwith Scotland.
ST types and geographic localization
Splitting the city into four divisions, north, south, east and west, revealed no localization of ST clusters. The total number of reported gonococcal cases found in deprived areas, depcats 6 and 7 (84 cases), was higher than the total number reported from middle class areas, depcats 3–5 (43 cases), and the more affluent areas, depcats 1 and 2 (18 cases).
DISCUSSION
Our study has shown that NG-MAST typing can support and offer a complementary and confirmatory tool for contact tracing and could potentially help establish partner networks when partner data are incomplete.
In all but one case, STs matched the contact information. A similar level of concordance was found in a study performed in London. 10 Discordant strains can be explained by incomplete reporting of contacts, the presence of mixed infection or rapid genetic strain variation.
The geographical distribution of STs commonly circulating in Scotland has been described, 7 however, on a smaller scale within the city of Glasgow; distinct spatial distribution of different strains of N. gonorrhoeae is not obvious. Meeting of sexual partners may be more likely to occur in central locations e.g. a city-centre club rather than in their residential area, allowing for geographical mixing of gonococcal strains.
In 1985, Potterat et al. 11 demonstrated the importance of social venues where sex partners meet. In our study, the self-completed interviews asked individuals where they socialized but this was localized to the city area rather than the name of an individual venue. The name of the venue (if applicable) where partners initially met could be asked as part of the contact history where full details of the persons involved are unknown. This may help in establishing transmission pathways of casual usually untraceable partners, and perhaps identify particular venues for venue-specific testing/health promotion.
Co-infection with Chlamydia trachomatis is more frequent in heterosexual men and women than in MSM. 12 Three of the eight exclusively heterosexually transmitted STs in our study were associated with chlamydial co-infection, but the remaining STs (24, 190, 236 and 478) that were heterosexually transmitted had no associated co-infection. Monitoring of this type of data could be potentially clinically relevant and have implications for standard co-treatment policies employed locally.
Continued linkage of clinical and behavioural data with STs over time could allow us to identify further changes in epidemiology. Previous research has shown close links between sexuality and specific STs. 13 ST210 has been associated with MSM, although in our study nearly two-thirds (7/11) with this type were heterosexual.
Recent relevance of NG-MAST typing data aiding local clinical practice was evident in Glasgow in 2004 when NG-MAST revealed an outbreak of ST470, which displayed azithromycin resistance. 14 NG-MAST helped in constructing and mapping a sexual network of this cluster where traditional partner notification methods had been unable to. Further afield in NSW, Australia the importance of rapidly identifying and investigating gonococcal clusters in an outbreak situation was shown. Public health measures were instituted quickly and the outbreak was interrupted. 15
Of the 18 new MAST types that were reported to the NG-MAST database 5 two of these 1311 and 1313 have been seen again in Scotland, both in 2006 and 2007. ST 1313 has also been reported in Greece. Online NG-MAST data do allow for a broader picture of gonococcal strains to be realized but is very dependent on the users of the system and some geographic areas are not covered at all and it therefore remains a useful but incomplete guide.
Our study was unable to show other associations to MAST type, possibly due to the small numbers involved and the multiple genotypes found, longer study may show associations. We did, however, demonstrate that NG-MAST strengthens alleged links between individuals. NG-MAST could also potentially help to identify social venues where venue-specific prevention initiatives could be used to help control N. gonorrhoeae infection if people frequently reported a specific partner meeting venue. For those unable to completely identify a sexual contact e.g. when only a first name is given, the venue where they met could be of value.
NG-MAST is a powerful tool in monitoring the epidemiology of gonococcal infection and it is of great benefit if NG-MAST data are available at the same time as culture confirmation to be of clinical value to those individuals involved. Since 2006, ST data have been reported back directly to GU medicine clinics in Scotland on a weekly basis to facilitate realtime monitoring of local changes in circulating gonococcal strains.