
Abstract
HIV-infected patients are at increased risk for persistent human papillomavirus (HPV) infection, the major cause of anogenital cancer. The present study describes the HPV prevalence in urine samples of 243 HIV-infected men and a control group of 231 men. HPV DNA was amplified by the SPF10 polymerase chain reaction primer set. The overall HPV prevalence in HIV-infected men was 27.5% compared with 12.6% in controls (P < 0.01). Infections with high-risk and multiple HPV genotypes were present in both groups. Differences were not statistically significant. A multivariate logistic regression model showed a decreased HPV prevalence associated with use of a nucleoside and a non-nucleoside reverse transcriptase inhibitor combination (P = 0.03). A trend was observed towards a higher HPV prevalence and a lower CD4 cell count. Further prospective studies are needed to determine the role of HPV DNA testing in urine in future screening programmes for anal cancer in men.
INTRODUCTION
Human papillomavirus (HPV) is the most common cause of sexually transmitted diseases (STDs) of viral aetiology worldwide. So far, approximately 130 HPV genotypes have been identified. About 40 genotypes have been detected in the anogenital area, and these are classified as low risk or high risk on the basis of their ability to cause cellular transformation in vitro and their association with cervical cancer. 1 The most prevalent high-risk genotypes are HPV 16, 18, 31, 33 and 45, whereas HPV 6 and 11 are examples of low-risk types because they are predominantly detected in benign lesions (e.g. genital warts).
About two-thirds of individuals who have sexual relations with an HPV-infected partner will become infected. In most HPV-infected individuals, the virus is cleared by the immune system in less than a year. 2 HIV-infected patients and other immunocompromised patients are at increased risk of persistent HPV infection due to chronic deviations in the immune system. 3,4
Persistent HPV infection is the major cause of invasive cervical cancer and its precursor lesions. 5 It has also been closely linked to other anogenital cancers, including anal cancer and certain penile cancers. 6 In men who have sex with men (MSM) with a history of receptive anal intercourse, the incidence of anal cancer was estimated to be 35 per 100,000 per year. 7 This is comparable with the incidence of cervical cancer before cervical cytology screening was implemented. In HIV-infected MSM, the incidence of anal cancer is even higher than in HIV-uninfected MSM. 7
Molecular biological methods to detect DNA in urine are routinely used to diagnose common STDs such as Chlamydia trachomatis and Neisseria gonorrhoeae. 8 Several studies showed that HPV DNA could be detected with high sensitivity in urine samples. 9,10 An advantage of detecting STDs in urine specimens is that it is a non-invasive sampling method and permits simultaneous detection of various infectious agents.
Although HPV has been studied extensively in women, data on male infection are limited. Because HPV infection in men is usually subclinical, there are a potentially large number of asymptomatic carriers who serve as reservoirs and vectors for the virus.
It is hypothesized that in the era of effective antiretroviral therapy (ART), the incidence of HPV-associated anogenital cancer in HIV-infected patients will increase as a consequence of prolonged survival combined with persistent deviations of the immune system. 11 Some authors propagate routine screening for specific populations including all MSM, regardless of HIV infection status. 12,13
The aim of the present study was to determine HPV prevalence in urine samples of HIV-infected men in the ART period. Furthermore, we investigated whether HPV prevalence was associated with CD4 cell count, HIV viral load or use of ART.
MATERIALS AND METHODS
Study population
Clean catch urine samples were obtained from HIV-infected men (n = 243) aged 24–74 years (mean 45 years) consecutively attending the outpatient HIV clinic at the Slotervaart Hospital from December 2005 until June 2006. All patients provided informed consent for the use of these materials for HPV research purposes. As a control group, urine samples from randomly selected men without known risk factors for HIV infection visiting the urology outpatient clinic (n = 231) were provided anonymously by the Microbiology Department at the Slotervaart Hospital. The study was approved by the Slotervaart Hospital research ethics committee.
HPV DNA amplification and detection
All samples were stored at −20°C until further processing. After DNA isolation, HPV DNA was amplified by the SPF10 polymerase chain reaction (PCR) primer set. Test characteristics and reaction conditions have been described before. 14 Each run was accompanied by several positive and negative quality control samples. During each PCR run, one negative control (water) and one positive control sample (HPV 18-positive cells) were tested. Amplification of a part of the beta-globin gene was used to assess the presence of human cells and the quality of target DNA. HPV-negative samples with a negative PCR result for the beta-globin gene were analysed again. HPV-negative samples with a positive beta-globin gene PCR were regarded as true HPV negatives. Amplification products were tested in a DNA enzyme immunoassay, a probe hybridization assay in a microtiter plate, to detect the presence of HPV DNA. This assay also included appropriate controls: one high positive, one low positive and a negative control. SPF10 amplimers from HPV DNA-positive samples were subsequently analysed using the HPV reverse hybridization assay (RHA). This assay comprises a membrane strip containing HPV type-specific oligonucleotides to specifically detect 25 HPV genotypes. HPV 6, 11, 34, 40, 42, 43, 44, 53, 54, 70 and 74 were considered low-risk types, whereas HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68 were considered high-risk types. Negative and positive controls were used to monitor the performance of the assay.
Statistical analysis
For statistical analysis, SPSS software (SPSS Inc., Chicago, IL, USA, version 13.0) was used. Data presented here were analysed using the chi-square test or Fisher's exact test. Multivariate logistic regression analysis was used to identify factors associated with HPV DNA positivity. A P value of 0.05 was considered the threshold level for significance.
RESULTS
The characteristics of HIV-infected men (n = 243) are shown in Table 1. In HIV-infected men the overall prevalence of HPV DNA was 27.5% (67/243) compared to 12.6% (29/231) in HIV-uninfected men (P < 0.01). HPV-positive samples were further genotyped by using the HPV RHA. The results of this genotyping are shown in Figure 1. Seventeen (10 HIV-infected and 7 HIV-uninfected men) of the 96 HPV-positive samples were positive in the HPV DNA screening assay but the RHA did not reveal a genotype. These samples are likely to contain HPV genotypes for which no probes are present in the RHA.
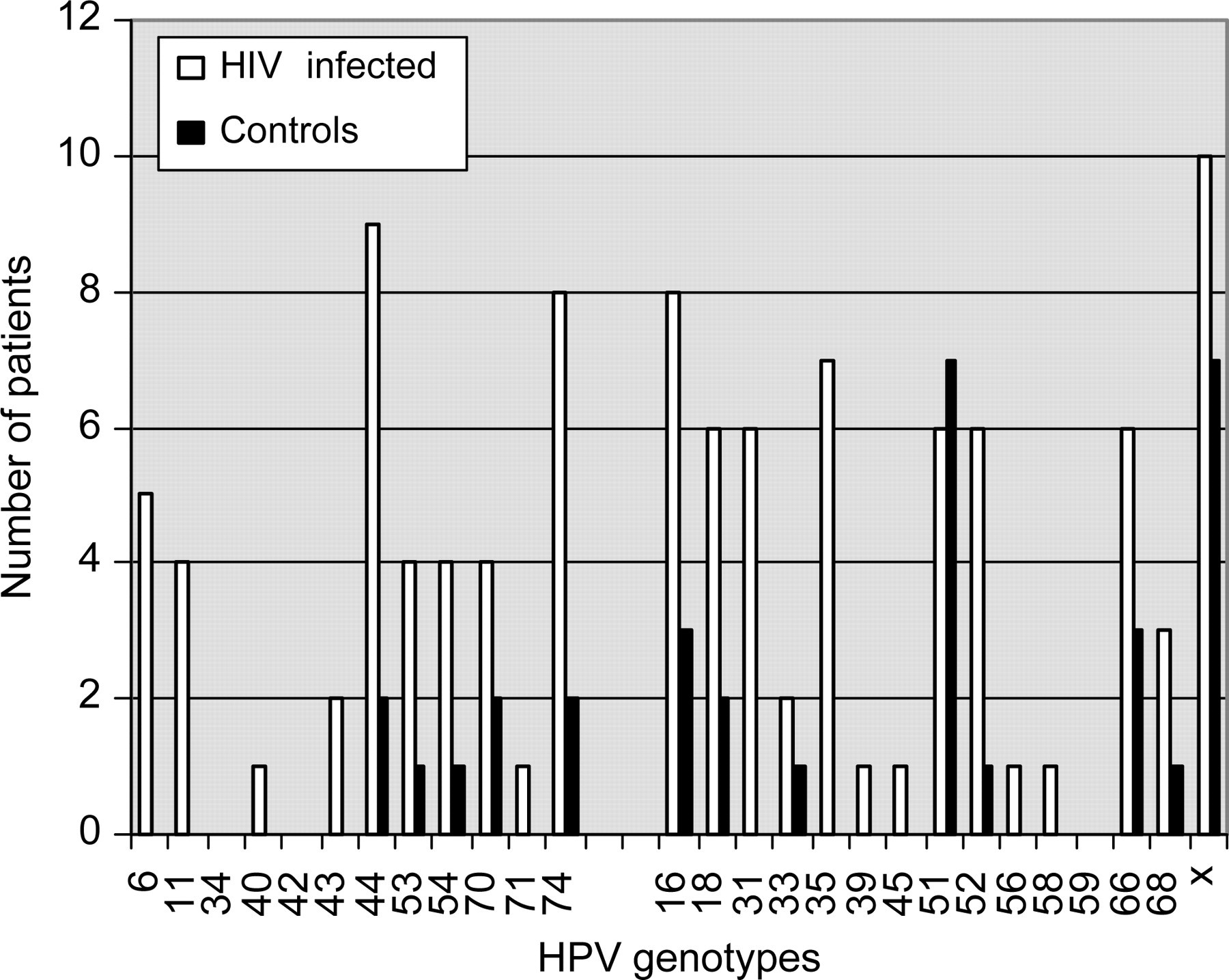
Distribution of human papillomavirus (HPV) genotypes in HIV-infected and HIV-uninfected men. HPV 6, 11, 34, 40, 42, 43, 44, 53, 54, 70, 71 and 74 (low-risk types); HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68 (high-risk types); X (undetermined HPV type)
Characteristics of HIV-infected men (n = 243)
ART = antiretroviral therapy; NRTI = nucleoside reverse transcriptase inhibitor; NNRTI = non-nucleoside reverse transcriptase inhibitor; PI = protease inhibitor
In both groups, high-risk HPV genotypes were detected. In HIV-infected men, 50.7% (34/67) were infected by a high-risk HPV genotype compared with 55.2% (16/29) in HIV-uninfected men (P = 0.69). The undetermined HPV genotypes were not taken into account. The number of multiple HPV genotypes present in HIV-uninfected men (4/29 multiple with two types) was lower than in HIV-infected men (17/67, ranging from 2 to 7 types) (P = 0.21).
In the HIV-infected men, we studied HPV prevalence according to CD4 cell count and HIV viral load. For this purpose we stratified these men into different subgroups of CD4 cell count (<200 × 106/L, 200–400 × 106/L and >400 × 106/L) and HIV viral load (<40 copies/mL and >40 copies/mL). The HPV prevalence in the different CD4 cell count subgroups was 44.4%, 32.1% and 22.9%, respectively. A trend was observed towards a higher HPV prevalence and a lower CD4 cell count. This trend reached significance when comparing HIV-infected men with a CD4 cell count <200 × 106/L and >400 × 106/L (P = 0.05). No association was found between HIV viral load and HPV prevalence.
The overall HPV prevalence in HIV-infected men using ART was 28.6% compared with 22.7% in HIV-infected men not using ART (P = 0.43). The specified HPV prevalence for the different ART regimens is 19.4% (21/108) for a nucleoside reverse transcriptase inhibitor (NRTI) and non-nucleoside reverse transcriptase inhibitor (NNRTI) regimen, 38.2% (21/55) for an NRTI and protease inhibitor (PI) regimen, 22.2% (2/9) for an NRTI, NNRTI and PI regimen, 47.8% (11/23) for an NRTI-only regimen and 50.0% (2/4) for a PI-only regimen. No significant differences in CD4 cell count and HIV viral load were observed between the different ART regimens.
To identify factors associated with HPV positivity and to correct for possible confounding factors, we performed a multivariate logistic regression analysis. In this model HPV was the dependent variable. CD4 cell count, HIV viral load, ART combination and age were entered as covariates. The only factor associated with a decreased risk of HPV positivity was an NRTI and NNRTI ART combination (P = 0.03).
DISCUSSION
We observed a significantly higher prevalence of HPV DNA (27.5%) in urine samples of HIV-infected men compared with HIV-uninfected men (12.6%) (P < 0.01). In previous studies the HPV prevalence in HIV-infected men varies from 0% to 93%. 3,15–17 It is difficult to compare the exact numbers from the different studies because a variety of clinical samples were analysed (e.g. biopsies, urine and smears) sampled from different sites (e.g. penis and anus).
Besides the significantly higher HPV prevalence in urine samples of HIV-infected men in our study, a trend was observed towards more infections with multiple HPV genotypes in HIV-infected men. Infections with multiple HPV genotypes, especially high-risk HPV genotypes, are regarded as independent risk factors associated with a higher chance of developing intra-epithelial neoplasia in women. 18
A trend was observed towards a higher HPV prevalence among HIV-infected men with lower CD4 cell counts. Some studies confirm this finding, while others reject it. 19,20 Owing to the effect of ART, only a small number of patients in our study population had a low CD4 cell count. We detected a higher HPV prevalence in patients treated with ART compared with patients not on ART. This finding seems paradoxical because by starting ART the immune system recovers and HPV infections can be cleared. In our opinion, this difference can be caused by persistent functional defects in the immune system and possibly by increased exposure to HPV due to differences in sexual behaviour between HIV-infected men ‘safely’ on ART and not on ART. However, we did not collect data on sexual behaviour because those data are prone to patient-based information bias.
In the logistic regression model, HIV viral load, CD4 cell count and age were all not significantly associated with HPV positivity. An NRTI and NNRTI ART combination, the most frequently used ART regimen in this cohort, was associated with a lower HPV prevalence. We have no clear explanation for this finding. The association could be based on chance. Another explanation could be that NNRTI has an intrinsic antiviral effect against HPV.
As shown in the present study and other studies before, urine is suitable for our HPV DNA detection system. 9,15 The SPF10 primer set amplifies a fragment of only 65 base pairs of the HPV genome. This short PCR fragment makes this assay a highly sensitive HPV detection method, which is suitable not only for pap smears but also for paraffin-imbedded tissue and urine samples.
In conclusion, the HPV prevalence in urine samples of HIV-infected men is high and infections with multiple genotypes are present. A trend was observed towards a higher HPV prevalence in patients with lower CD4 cell counts. Owing to their prolonged survival and persistent deviations in the immune system, HIV-infected men are at risk for developing HPV-related anogenital malignancies and screening programmes may be warranted. Further prospective studies are needed to determine the role of HPV DNA testing in urine in screening programmes and to compare it with HPV DNA testing in anal swabs and biopsies and results of cytology and histology.