
Abstract
Acquired lymphoedema of the vulva is induced by impaired lymph flow. We present the case of a 35-year-old woman having lymphoedema of the vulva following pulmonary tuberculosis, which she had developed four years back for which she had taken a full course of antitubercular treatment for nine months from the Chest and Tuberculosis department. The biopsy taken from the perianal swellings showed hyperkeratosis and acanthosis with multiple dilated lymph specs.
INTRODUCTION
Genital elephantiasis is an important medical problem in the tropics and usually affects the young and productive age group. Lymphoedema of the genital region is relatively uncommon, but is extremely uncomfortable and distressing for patients who suffer from this condition. It can affect men and women alike, but is seen more frequently in men due to the anatomical differences between genders and the effects of gravity. Around 10% of people who develop leg oedema will have associated genital swelling, but some patients can have genital oedema alone.
In some circumstances, genital oedema can occur acutely due to trauma or cellulitis and may be able to resolve completely by itself. Far more usual, however, is chronic genital oedema, which is unfortunately irreversible, but can be controlled and reduced through appropriate lymphoedema management. The main cause of genital oedema is due to either primary or secondary lymphoedema.
The main reasons for primary genital lymphoedema are that the lymph vessels are absent or reduced in number or simply do not work as well as they should, i.e. functional failure. Secondary lymphoedema is frequently seen due to infectious diseases such as filariasis. This can lead to gross elephantiasis of the penis and scrotum. It has been reported that up to 70% of patients treated for carcinoma to the vulva will have lower body swelling. The other causes include sexually transmitted diseases (STDs) such as lymphogranuloma venereum (LGV) and donovanosis as well as malignancies. Radiotherapy to the lymph nodes in the groin or abdominal region can also cause genital lymphoedema. The incidence also increases if there has been surgery and radiotherapy plus episodes of cellulitis.
CASE REPORT
A 35-year-old woman, who had been married for 20 years, reported to the surgery outpatient department with complaints of a vulval swelling (Figure 1) since the past 18 months and multiple sinuses (Figure 2) around the anus for the last 21 days. On examination a large, pendulous mass of hypertrophied tissue hanging down and obstructing the vulval cleft was observed. The swelling arose from both labia majora. The mass was pyriform in shape, and the surface was smooth and shiny. The introitus, clitoris and other parts were found to be normal. There was ulceration on the dependent part of the swelling on one side. On examination, no inguinal, axillary or cervical lymph nodes were palpable. As stated by her, she had developed pulmonary tuberculosis about four years back, for which she had taken a full course of antitubercular treatment for nine months from the Chest and Tuberculosis (TB) department.

Woman with massive vulval lymphoedema

Perineal view showing vulval oedema and multiple perianal fistulas
The patient is a housewife with two sons. She and her spouse denied any extramarital exposure. No one in the family had any history of TB. She was moderately built and afebrile at the moment. There was pallor, and general physical and systemic examinations did not reveal any other abnormality. Vaginal, urethral and anal orifices appeared normal. Haemoglobin was 9.8 gm%; total leukocyte count was 8600 cells/mm3; erythrocyte sedimentation rate was 88 mm at the end of the first hour; Tridot screening for HIV, Venereal Disease Research Laboratory (VDRL) and serological tests for other STDs were negative. The Mantoux test was strongly positive with blister formation (Figure 3). A sputum sample was negative for acid-fast bacilli. X-rays of the chest and pelvic region were normal. The biopsy was taken from the perianal swellings, which showed hyperkeratosis and acanthosis (Figure 4). Multiple dilated lymph spaces were seen in the upper dermis.

Flexural aspect of the arm showing positive Mantoux test (blister formation)
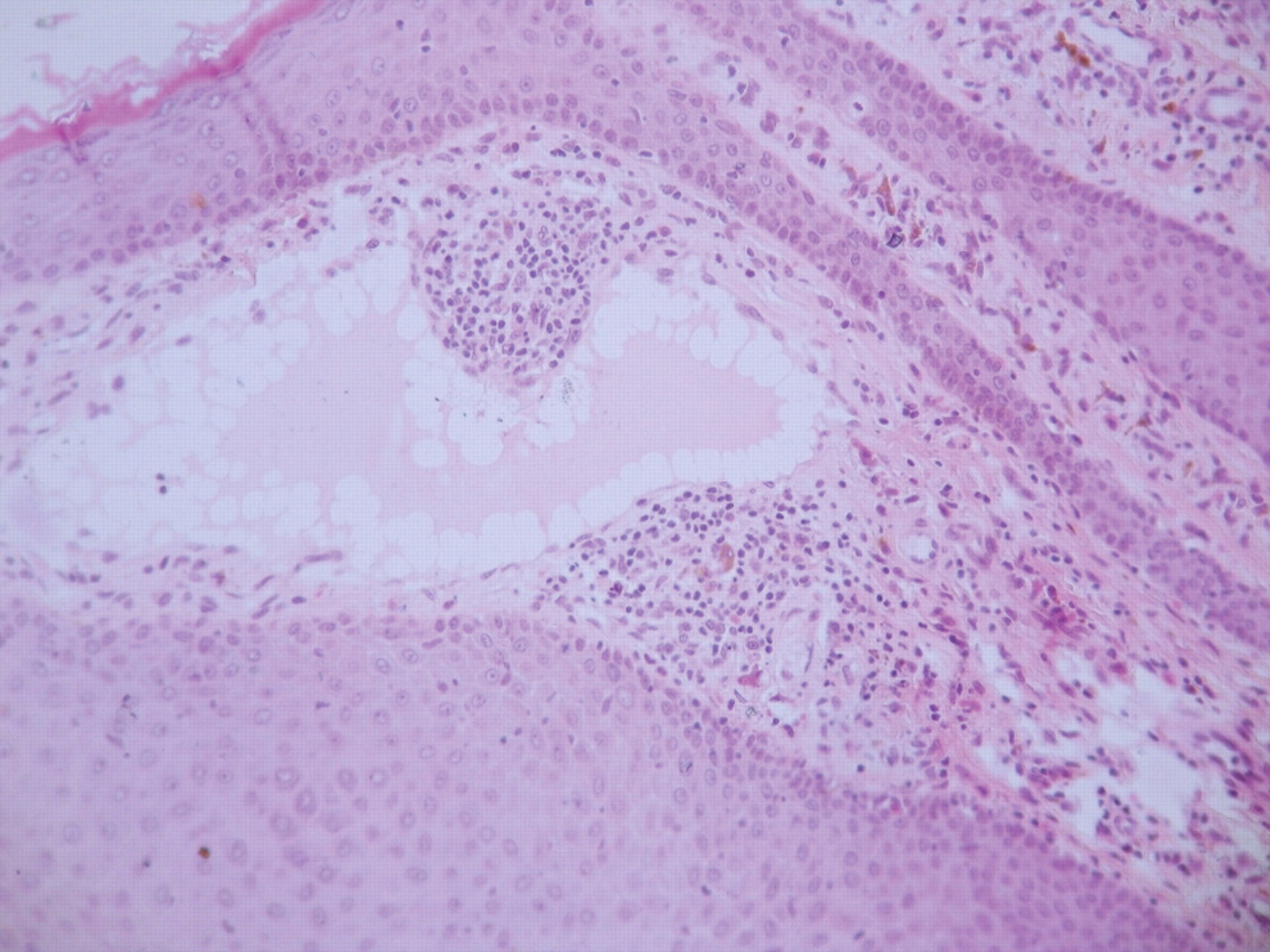
Well-formed typical epithelioid granuloma with typical Langerhans giant cells within endometrial stroma. Chronic inflammatory cells can be seen around granulomas
The patient has been referred for a vulvectomy by a plastic surgeon.
DISCUSSION
Genital elephantiasis is defined as grotesque enlargement of the genitals due to lymphatic channel obstruction from various causes. Although the term ‘elephantiasis’ was originally used to describe the elephant-like appearance of legs, the term was subsequently used to describe similar enlargement of the arm, chest, breast, penis, scrotum and vulva. 1 The term ‘esthiomene’ is applied when genital elephantiasis is associated with ulceration in genital labia in females 2,3 and is derived from a Greek verb, which means ‘to eat’ and evokes the idea of something being gnawed, eroded or ulcerated. 4 The majority of the cases are due to filariasis; however, a small but significant proportion of patients develop genital elephantiasis due to bacterial sexually transmitted infections (STIs), mainly LGV and donovanosis. STI-related genital elephantiasis should be differentiated from elephantiasis due to other causes, including filariasis, tuberculosis, haematological malignancies, and iatrogenic or dermatological diseases. 5 Irrespective of aetiology, the basic process remains the same, i.e permanent obstruction of the lymphatic channels leading to lymphatic stasis, which stimulates the growth of fibroblasts leading to destruction of lymph nodes, which causes lymphoedema and elephantiasis.
In a patient with genital elephantiasis, the importance of taking a proper history and thorough clinical examination cannot be overemphasized as it may help to find the cause for the elephantiasis. Rarely, genital elephantiasis has also been described as a complication of syphilis and infection with non-LGV strains of Chlamydia trachomatis. Laboratory investigations such as microscopy of tissue smear and the nucleic acid amplification test for donovanosis and serology and polymerase chain reaction (PCR) for LGV may help in the diagnosis. However, in the absence of laboratory facilities in endemic areas, diagnosis largely depends on clinical characteristics.
Elephantiasis associated with tuberculosis closely resembles elephantiasis due to LGV, as both are associated with inguinal lymphadenitis. However, a reactive Mantoux test, suggestive histopathology, isolation of Mycobacterium tuberculosis by PCR or culture and response to antituberculosis therapy are confirmatory for tuberculosis. 6,7 In the context of tuberculosis, it must be remembered that the disease can also produce pseudoelephantiasis (i.e. elephantiasis of genitalia secondary to genital pathology) with a similar clinical presentation. 8,9
Genital elephantiasis is a significant medical problem and persons affected may become a major burden to their family and community, especially when the disease interferes with their economic livelihood. At present, surgery is the only effective option for patients like this one, in whom the disorder is disabling, persistent and psychologically devastating.