
Abstract
Overall HIV test coverage among pregnant women in Brazil is 62%, but only 41% in northeastern Brazil. We aimed to identify risk factors for unawareness of HIV status among pregnant women and determine test coverage up to 14th week of pregnancy. We conducted a case-control study in a reference maternity hospital for high-risk pregnancy in Recife, where 485 puerperae were interviewed about their knowledge of results of HIV testing, biological, sociodemographic and healthcare data. Cases were those who were not aware of their HIV status and controls were those who were. Only 21.65% stated that they were unaware of their HIV status during pregnancy (78.35% coverage); however, test results were recorded on an antenatal card in only 48.35%. Only 22% received the result by the 14th week of pregnancy. Unawareness was associated with low schooling (odds ratio [OR] = 2.92; P = 0.006); living outside the state capital's metropolitan region (OR = 4.11; P = 0.001); test performed in the third trimester (OR = 11.6; P = 0.000); and lack of counselling (OR = 2.31; P = 0.022) in multivariate analysis. In conclusion, there has been a considerable delay in having an HIV test. Conflict of Information obtained by interview and that on the antenatal card raises questions about deficiencies in antenatal care or lack of comprehension about the HIV test.
Introduction
The classic study by Connor et al. 1 in 1994 (PACT 076) showed that the use of zidovudine during labour and following delivery by the newborn up to 42 days after birth, together with no breastfeeding, achieved a reduction in the risk of vertical HIV transmission from 25.5% to 8.3% (67.5%).
In 1998 and 1999, it was shown that the risk of vertical HIV transmission could be further reduced to rates of 0.8–2% if elective caesarean section was associated with the previous measures.2,3
In 2002, a prospective cohort study showed better results with the use of combined highly active antiretroviral therapy (HAART) than with zidovudine monotherapy: vertical HIV transmission rates were 10.8% (confidence interval [CI] 8.2–12.6%) using zidovudine monotherapy and 1.2% (CI 0–2.5%) using HAART. 4
In 1994, the Centers for Disease Control recommended using zidovudine for infected pregnant women in the United States. 5 In 1995, the Brazilian Ministry of Health published specific regulations regarding prophylaxis against vertical HIV transmission, thereby establishing this as a priority within the National STD/AIDS Program. 6
Brazil put these measures into practice in 1997 (Ministry of Health, ordinance no. 874/97), making diagnostic tests, antiretrovirals, recommended delivery methods, maternal milk substitutes and specialized follow-up freely available for HIV-infected mothers and exposed newborns. Pregnant women who did not require treatment for their own disease were advised to start prophylaxis with combined HAART against vertical HIV transmission from the 14th week of pregnancy 7 and those pregnant women who required treatment for their own disease were advised to start it irrespective of the stage of pregnancy.
The adoption of the measures included in the Ministry of Health regulations 7 led to a reduction of approximately 50% in the number of AIDS cases resulting from vertical transmission between 1996 and 2005 (from 1228 to 648 cases). 8 However, the vertical transmission rate in Brazil has still not come down to desired levels.
One of the major obstacles is the situation in which no HIV testing is performed or the results remain unknown during pregnancy, as shown by the Pregnant Woman Sentinel Study of 2006. This study found that the test coverage rate was of the order of 62% for the whole of Brazil, with large regional differences. The coverage was 86% in southern Brazil, 74% in the southeastern region and 70% in the centre-west region. In contrast, the northern and northeastern regions presented coverages of 46% and 41%, respectively. This study also showed that the coverage was greater in municipalities with more than 400,000 inhabitants (71%) and lower in municipalities with fewer than 50,000 inhabitants (52%). 9
A low coverage of HIV testing during pregnancy has the direct repercussion of higher vertical HIV transmission rates. The national mean was 6.8% in 2004, with regional differences ranging from 5.1% in the centre-west region to 11.8% in the northern region and 8.9% in the northeastern region. 10
In 2007, the Brazilian Ministry of Health launched a national plan for reducing vertical HIV and syphilis transmission, with tiered regional targets for reducing the vertical HIV transmission rate by 2011 to 2.1% in the centre-west region, 6.6% in the northern region and 3.6% in the northeastern region. Among other measures, the plan recommends that HIV testing should be conducted in the first and third trimesters of pregnancy. 11
The low coverage achieved by HIV testing in the northeastern region despite the importance of early diagnosis of HIV infection among pregnant women was the stimulus for conducting the present study. Its aim was to identify the frequency of unawareness of HIV serological status during pregnancy and the risk factors for such unawareness among a group of women admitted for delivery at a hospital in northeastern Brazil. It also sought to identify how frequently the pregnant women knew their HIV test results by the 14th week of pregnancy.
Methods
This study was conducted between April and October 2007 in the maternity department of Hospital Agamenon Magalhães (HAM), Recife, Brazil. This is a reference hospital for high-risk pregnancy and provides medical care for pregnant women from various cities in the State of Pernambuco, performing an average of 3000 deliveries per year.
Unawareness of HIV serological status during pregnancy was defined as a situation in which no HIV testing had been carried out during the pregnancy or, even if it had been carried out, there had not been any access to the test results up to the time of admission for delivery.
The study consisted initially of a cross-sectional survey to determine the frequency of unawareness of HIV serological status during pregnancy and the degree of knowledge of the results from HIV testing by the 14th week of pregnancy. After ascertaining these data, the investigation proceeded as a case-control study in which cases were those pregnant women who were unaware of their serological HIV status and controls were those who were aware of their serological status up to the time of admission for delivery.
Interviews were held with 485 puerperae who had been admitted for delivery, using a standardized questionnaire with closed questions that had previously been tested in a pilot study. Data on antecedents of maternal HIV infection and gestational age were obtained from the medical records of the puerperae and their newborns. Their antenatal cards were checked to see whether there was any record of HIV testing.
The study subjects were selected by means of simple random sampling, with replacements, from the obstetric events book in the delivery room. The exclusion criteria were previous diagnosis of HIV infection, abortions and/or miscarriages, or maternal pathological conditions that would impair questionnaire application.
The sample was calculated based on an analysis of the first 150 questionnaires, taking an alpha error or 5% and a sample power of 80%, on the basis of the lowest odds ratio (OR) encountered, which was 2.37 (for the variable ‘knowledge of the purpose of HIV testing’), and the corresponding frequency of exposure among the controls, which was 18.7%. Taking proportions of one case for every three controls, the calculation yielded a ratio of 79:237. The final sample was composed of 105 cases and 380 controls.
For the risk analysis, the dependent variable was taken to be unawareness of HIV serological status during pregnancy. The independent variables were biological, reproductive, Sociodemographic, health care and health information factors.
The project was approved by the HAM Ethics in Research Committee (protocol number 16/2007). The interviews were held after a full explanation about the study had been given and after the subjects had signed an informed consent statement.
Descriptive analysis was performed on all variables. Following this, OR were used as an association measurement (with 95% confidence intervals, CI), and the statistical significance of such associations was analysed using the chi-squared test (P < 0.05). Multivariate analysis was performed for each block separately. All data analyses were performed using the Epi Info version 6.04 and STATA version 9 software.
Results
According to information from the interviewees, 51% were from cities with more than 400,000 inhabitants (Recife and Jaboatão dos Guararapes) and 98% had had antenatal care, of whom 68.6% started this during the first trimester and 68.2% had had six or more consultations. Of the total number of interviewees, 11.13% (54 women) had not had HIV testing and 10.5% (51) had not had access to the results; a total of 21.65% of the women (105) were thus unaware of their HIV serological test results during pregnancy. Of the 98% (475 women) who had had antenatal care, testing was requested for 94.73% (450). However, 75.4% were not asked whether they wished to have the test.
Of the 78.14% (379 women) who said they knew the results of HIV testing performed during their pregnancies, 87.42% brought their antenatal card. The test results were recorded on this card in only 48.35% of the cases. Of the women who said they had undergone the test, only 22% (84) said they knew the results by the 14th week of pregnancy. However, considering only those who had the test in public hospitals or health posts, this percentage dropped to 15.4% (54).
Biological, reproductive and sociodemographic characteristics of the puerperae in relation to unawareness of HIV serological status during pregnancy, Recife, 2007
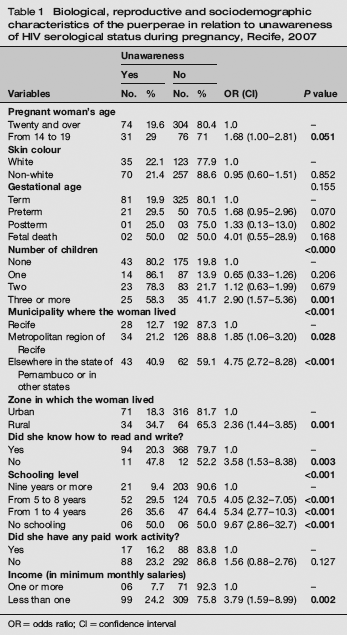
OR = odds ratio; CI = confidence interval
Socioeconomic characteristics of the head of household of the puerperae in relation to unawareness of HIV serological status during pregnancy, Recife, 2007
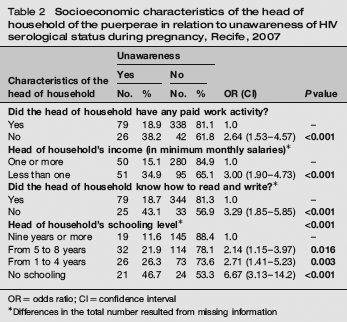
OR = odds ratio; CI = confidence interval
Differences in the total number resulted from missing information
Health-care characteristics of the puerperae interviewed; in relation to HIV serological status during pregnancy, Recife, 2007
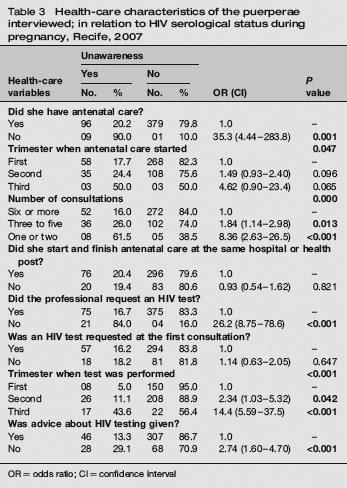
OR = odds ratio; CI = confidence interval
Association between unawareness of HIV serological status during pregnancy and health information about HIV among the puerperae interviewed, Recife, 2007
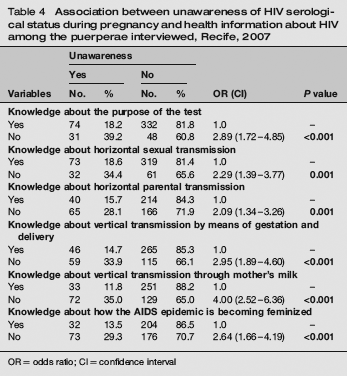
OR = odds ratio; CI = confidence interval
Final model for the association between the characteristics of the puerperae interviewed and unawareness of HIV serological status during pregnancy, Recife, 2007

OR = odds ratio; CI = confidence interval
Discussion
One of the limitations of the present study is that it was conducted in a high-risk maternity hospital. Thus, the population analysed may have had better antenatal medical care than what the general population receives.
A number of wide CIs in our study resulted from the size of the sample. However, increasing the sample size would not change the statistical significance found: rather, it would contribute towards increasing the precision, i.e. towards obtaining narrower CIs.
From the information provided by the puerperae, it was shown that the rate of unawareness of HIV test results during pregnancy was 21.65% (which corresponded to a coverage of 78.35%) and that only 22% of the pregnant women knew the test results by the 14th week of their pregnancy. This figure fell down to 15.4% when only the women who had the test at a public hospital or health post were considered.
It was also shown that the risk of unawareness of HIV serological status during pregnancy was three times greater if the pregnant woman had less than nine years of schooling and four times greater if she lived outside the metropolitan area of the state capital. Performing the test only in the third trimester of pregnancy increased the risk of unawareness by a factor of at least four. The risk of unawareness was around 2.5 times greater if the pregnant woman was not advised about the importance of HIV testing during pregnancy.
The coverage of HIV testing that was ascertained from information provided by the women was 78.35%. This percentage is higher than that reported for the northeastern region in the Pregnant Woman Sentinel Study of 2006, which was 40%. 9 However, the latter study was based on test record data on the antenatal card, and not on information from the puerperae. This methodological difference may explain the difference in the results. Using the test record data on the antenatal cards of the present study (these cards were brought in by 87.42% of the puerperae, although test records were only found on around 48.35% of them), the percentage coverage was around 40%, i.e. similar to that found in the Pregnant Woman Sentinel Study of 2006. 9 This discrepancy in evaluating the coverage between the information provided by the puerperae and the data on the antenatal card is clear evidence that at present there is no gold standard for obtaining this assessment. Some reasons could explain this discrepancy, which occurred in a large proportion of cases: the questionnaire was not sufficiently clear to be understood by this population; the pregnant women did not know the meaning of HIV test and were not sufficiently encouraged to ask the investigator; the HIV examinations were done, but were not recorded in the antenatal card by the healthcare professionals; the HIV examinations were done, but the results were not available, causing confusion in the pregnant woman? Unhappily, this discrepancy was detected after the study was completed, not allowing to determine its origins.
Souza Júnior et al. 12 and Szwarcwald and Souza Júnior 13 took information from pregnant women to evaluate the coverage of HIV testing during pregnancy. For northeastern Brazil, they, respectively, found coverage rates of 24% and 31.1%, which are closer to what was found in the Pregnant Woman Sentinel Study of 2006 9 and thus below what we found. Therefore, the greater coverage that we found, which was an unexpected finding from the study, may perhaps be explained by the fact that the sample came from a reference maternity hospital for high-risk pregnancy and also the fact that 51% of the sample came from cities with more than 400,000 inhabitants, in which a test coverage of 70% during pregnancy has been shown in a previous study. 9
If we consider only the information of the questionnaire, the level of coverage of 78.35% is similar to the levels found in the southern region of Brazil and in developed countries. In the United States, Sanson and Anderson 14 used data from a national reproductive health study conducted in 2002 and found that only 69% of the interviewees who had been pregnant during the preceding 12 months had had an HIV test during their pregnancy. In a study among obstetricians registered with the Royal Australian and New Zealand College of Obstetricians and Gynecologists, in which 70% of all Australian obstetricians participated, Giles et al. 15 recorded that only 70% of them said that they always offered HIV testing to the pregnant women. However, despite the good test coverage, these data demonstrate lost opportunities for prophylaxis against vertical HIV transmission, even in developed countries.
On the other hand, the high lack of awareness of HIV serological status before the 14th week of pregnancy in our study was notable. This point had not been analysed in previous studies. It is an important point, since an early start to antiretroviral treatment enables effective reduction of the viral load to undetectable levels, 16 which reduces the risk of vertical transmission to 1% (CI 0.4–1.9%) by the end of pregnancy and at the time of delivery.4,16–18 Even though it has been shown that starting the use of antiretrovirals at later stages of pregnancy16,17 or even at the time of admission for delivery 18 may also reduce vertical HIV transmission, an early start is better.4,19,20 It can therefore be seen that, although our study population presented a good test coverage, opportunities for intervention regarding vertical HIV transmission are still being lost. Efforts need to be made towards implementing HIV tests at an early stage of pregnancy, with results issued promptly.
Performing HIV testing during the third trimester was associated with unawareness of HIV serological status during pregnancy. This suggests that there were delays in handing over the test results, which once again indicates the need to implement measures to speed up this process or a need to bring in rapid tests of high sensitivity and specificity into the antenatal routine.
Low schooling levels and residence in a municipality outside the metropolitan region of Recife were associated with low coverage of HIV testing in the study group. This was also shown by Souza Júnior et al. 12 and Szwarcwald and Souza Júnior, 13 and in the Pregnant Woman Sentinel Study of 2006, 9 in which the coverage rate for HIV testing during antenatal care was 48% among pregnant women with less than four years of schooling and 70% among those with 11 or more years of schooling. This is also of concern, since it is precisely this population that is most vulnerable to HIV infection. In a study carried out in Rio de Janeiro, Fernandes et al. 21 found that 67.5% of the HIV-infected mothers had had less than nine years of schooling. Therefore, specific strategies for this more vulnerable population must be prioritized.
The low coverage of HIV testing outside the metropolitan region of Recife, which was also shown in the Pregnant Woman Sentinel Studies of 2002, 12 2004 13 and 2006 9 for small-sized municipalities, together with the spread of the HIV/AIDS epidemic to these non-metropolitan municipalities, increases the risk of vertical transmission of this virus. It also shows the difficulties in accessing healthcare provision in small-sized municipalities.
Requesting HIV testing without previously consulting the pregnant woman about whether she wanted to have it occurred in 75.4% of the cases. This was contrary to the guidelines issued by the World Health Organization 22 and Brazilian Ministry of Health 23 and it shows the absence of counselling at the time of making the request.
Lack of knowledge about the importance of HIV testing during pregnancy increased the risk of unawareness of HIV serological status by a factor of around 2.5. This shows the importance of counselling at the time the test is requested. Goldani et al. 22 evaluated 1658 pregnant women in Porto Alegre, in southern Brazil, and found that for 59% of them, HIV testing was requested without providing any counselling, and that the pregnant women coming from less privileged social groups were given counselling less frequently. In a study carried out at family healthcare units in Fortaleza, State of Ceará, northeastern Brazil, in 2005, Araújo observed that counselling before and after HIV testing was not given by the health professionals of those units. 24
Among other measures, HIV counselling includes joint assessment with the individual of the risks of HIV acquisition to which this person is exposed, guidance on the means of virus transmission (including vertical transmission in the case of pregnant women) and guidance on reducing the risks of acquiring the virus or re-exposure.22,23 Thus, when counselling is not given, an important opportunity for intervening in the HIV transmission chain is lost.
Conclusion
Taking the information from the puerperae as reference, this study demonstrated an HIV test coverage rate during pregnancy higher than that obtained previously for northeastern Brazil, in conflict with the records on antenatal card. However, in whatever source of information, HIV test coverage up to the 14th week of pregnancy was notably low, particularly when only the women who had the test at a public hospital or health post were considered. This represents a missed opportunity for obtaining the best results in terms of prophylaxis against vertical transmission and the necessity of focusing efforts in performing the test more rapidly. This can be achieved by testing at an earlier stage or by using new technology such as fast HIV testing.
Finally, there is a more vulnerable population, with lower levels of schooling and living in small-sized municipalities, that needs to be the preferential target of campaigns for inclusion in testing programmes.