
Abstract
Thirty-six HIV-1 cases had been reported by December 2007 in Mongolia. Therefore, Mongolia has been regarded as a very low HIV-1 epidemic country, although the surveillance system is not fully developed. The aim of this study was to evaluate the risk status of HIV-1 infection in Mongolia. A total of 1415 blood samples from high-risk populations including female sex workers, men who have sex with men, mobile men, tuberculosis patients and male sexually transmitted infection (STI) clinic clients and 1050 samples from healthy controls were collected. The seroprevalences of anti-HIV-1/2, anti-Treponema pallidum, hepatitis B surface antigen (HBs Ag), anti-hepatitis C virus and hepatitis B surface antibody in the high-risk populations were 0%, 23.1%, 15.5%, 8.0% and 48.2%, and those in the controls were 0%, 3.1%, 14.7%, 4.4% and 44.4%, respectively. HIV-1 prevalence is currently low. However, according to the high prevalence of STIs in the high-risk populations, the risk status for HIV-1 infection is estimated to be high.
INTRODUCTION
Mongolia is located in Central Asia bordered by Russia and China. The population of Mongolia is 2635 million, of which 61.0% live in cities and the remaining are nomadic. 1 Geographical conditions and a very low population density make communication, transport and health service provision difficult. Mongolia has witnessed radical changes in its economic and social policies since the democratic revolution of 1990. Along with independence from the former Soviet Union and loss of Soviet support, there has been an increase in unemployment, alcoholism and prostitution and a steady increase in the prevalence of sexually transmitted infections (STIs) and other communicable diseases. 2–8 A recent study demonstrated that syphilis, gonorrhoea and trichomonas were detected in 57 (43%), 18 (14%) and 37 (28%) subjects, respectively, among 132 low-income female commercial sex workers (FSWs) in Mongolia. 9 Mongolia also has a high prevalence of hepatitis B and C viral infection. In a previous study, hepatitis B surface antigen (HBs Ag) and antibodies to hepatitis C virus (anti-HCV) were detected in 24 (10%) and 41 (16%) subjects, respectively, among 249 apparently healthy individuals in Mongolia. 10 However, most of these data were obtained from convenient or non-generalized samples. There is a lack of information regarding exposures and the burden of diseases in the high-risk populations for HIV and STIs. High-risk populations such as FSWs and their sexual contacts with high rates of STIs are important populations contributing to the transmission of HIV and other STIs in developing countries. 11–13
Since 1992, when data on HIV/AIDS began to be compiled in Mongolia, there had been only five cases reported as of December 2004. Mongolia is considered as an HIV/AIDS low-prevalence country. However, annual new cases of HIV/AIDS have been increasing in recent years. For example, 11, 9 and 11 new cases were detected in 2005, 2006 and 2007, respectively. Among them, 22 (61.1%) cases were men who have sex with men (MSM), seven (19.4%) were heterosexually transmitted and six (16.7%) were FSWs (Mongolian National Center for Communicable Diseases [NCCD], unpublished data). Owing to the lack of a sound surveillance system, the actual situation is uncertain. The primary objective of this study was to evaluate the current risk status of HIV-1 among high-risk populations in Mongolia, examining the seroprevalence of other STIs concomitantly. These data are crucial for taking future preventive measures against HIV-1 infection.
METHODS
Study design and study population
This study was conducted from September through December 2007. The study protocol was approved by the ethics committees of the International Medical Center of Japan (H19-448) and of the Ministry of Health, Mongolia. After explaining this study and obtaining informed consent, blood samples were collected anonymously from both high-risk and healthy control populations in Ulaanbaatar (the capital city of Mongolia) and four aimags including Dornod, Huvsgul (borders of Russia), Dornogobi (a border of China) and Darkhan-Uul (Figure 1). A total of 2465 samples were collected: 1415 samples from high-risk populations and 1050 samples from healthy control populations. The high-risk populations included FSWs, MSM, mobile men, tuberculosis (TB) patients and male STI clinic clients. The number of samples in each population and demographic characteristics are listed in Table 1.

A map of Mongolia. Blood samples were collected from the capital city Ulaanbaatar and four aimags (provinces), such as Darkhan-Uul, Huvsgul, Dornod and Dornogobi. Asterisks indicate the sites where blood samples were obtained
Demographic characteristics of persons who gave blood samples
FSW = female commercial sex worker; MSM = men who have sex with men; TB = tuberculosis; STI = sexually transmitted infection
Cluster sampling was used for FSWs in locations such as bars, nightclubs, sauna and massage parlours serving as clusters. MSM were sampled only from Ulaanbaatar city, due to the limited data on MSM in other areas of the country. Mobile men were sampled from Ulaanbaatar city and Dornogobi aimag (province), along major road and rail networks and areas such as truck stops and checkpoints at borders. As for TB patients, those who were diagnosed with TB for the first time during the sampling period were enrolled. A male STI clinic client was defined as one who attended public STI clinics during the sampling period. A healthy control group included youth and blood donors. Youth was defined as unmarried, 15–35 years old students in college or university of both sexes. The blood donors were selected in health facilities during the sampling period.
Specimen collection and serology
All sera were stored below −20°C until use. Sera were tested for antibodies to HIV-1/2 (anti-HIV-1/2), Treponema pallidum (anti-TP), hepatitis B surface antiboby (HBs Ab), and hepatitis C virus (anti-HCV) and HBs Ag by using the chemiluminescent enzyme immunoassay (CLEIA) (Lumipalus, Fujirebio, Tokyo, Japan) according to the instructions provided by the manufacturer. Seropositive samples for anti-HIV-1/2 by CLEIA were further confirmed by chemiluminescent immunoassay (Architect, Abbott Laboratories, Abbott Park, IL, USA) and a Western blot for the final diagnosis. All laboratory analyses were performed at the AIDS Clinical Center, International Medical Center of Japan.
Statistical analyses
Differences among high-risk and/or healthy control populations were examined by the Fisher's exact test. Univariate logistic analyses were used to determine the odds ratios (OR) with corresponding 95% confidence intervals (CI). All analyses were conducted using the Stat View software version 5.0 (SAS Institute, Cary, NC, USA). A P value of <0.05 was considered statistically significant.
RESULTS
The seroprevalences of anti-HIV-1/2, HBs Ab and Ag, anti-HCV and anti-TP of each group of the high-risk and healthy populations are presented in Table 2. None of the anti-HIV-1/2-positive samples was detected in this study. The prevalences of HBs Ag and HBs Ab in the high-risk population, including among each high-risk group, were not different compared with those in the healthy control. In contrast, the prevalences of anti-HCV (8%) and anti-TP (23.1%) in the high-risk population were significantly higher than those in the healthy control. The ORs of anti-HCV and anti-TP comparing between the high-risk population and the healthy control were 1.9 (95% CI: 1.3–2.7, P < 0.001) and 9.3 (95% CI: 6.4–13.4, P < 0.0001), respectively. The prevalences of anti-HCV in MSM and TB patients were higher than those of other risk groups. The prevalences of anti-TP in FSWs (39.5%) and MSM (30%) were surprisingly high.
Seroprevalence between high-risk and healthy controls in Mongolia
FSW = female commercial sex worker; MSM = men who have sex with men; TB= tuberculosis; STI = sexually transmitted infection; OR = odds ratio; CI = confidence interval; HBs Ag = hepatitis B surface antigen; HBs Ab = hepatitis B surface antibody; TP = Treponema pallidum; HCV = hepatitis C virus
Geographical differences of seroprevalence are shown in Table 3. Again, there were no significant differences of the prevalence of HBs Ab and Ag in different regions of specific high-risk groups. However, incidences of anti-HCV and anti-TP had some differences in different regions of the specific groups. A striking feature was that the prevalence of anti-TP in Ulaanbaatar FSWs was 54.7%.
Seroprevalence of HBV, HCV and syphilis among a high-risk population by residence
HBV= hepatitis B virus; HCV = hepatitis C virus; TP= Treponema pallidum; FSW = female commercial sex worker; MSM = men who have sex with men; TB = tuberculosis; STI = sexually transmitted infection; OR = odds ratio; CI = confidence interval; HBs Ag = hepatitis B surface antigen; HBs Ab = hepatitis B surface antibody
The prevalence of HBs Ab was high. However, there were no differences in the prevalence between high-risk and healthy control populations over the country. One reason was that a hepatitis B virus (HBV) vaccination programme in childhood has been implemented 18 years ago. Therefore, we divided the subjects into two age-related groups (below 18 years and over 20 years) and analysed the seroprevalence of HBs Ab (Figure 2). There were no differences between the high-risk and healthy control populations in both age-related groups. However, in both high-risk and healthy control populations, higher age groups had significantly higher prevalence.
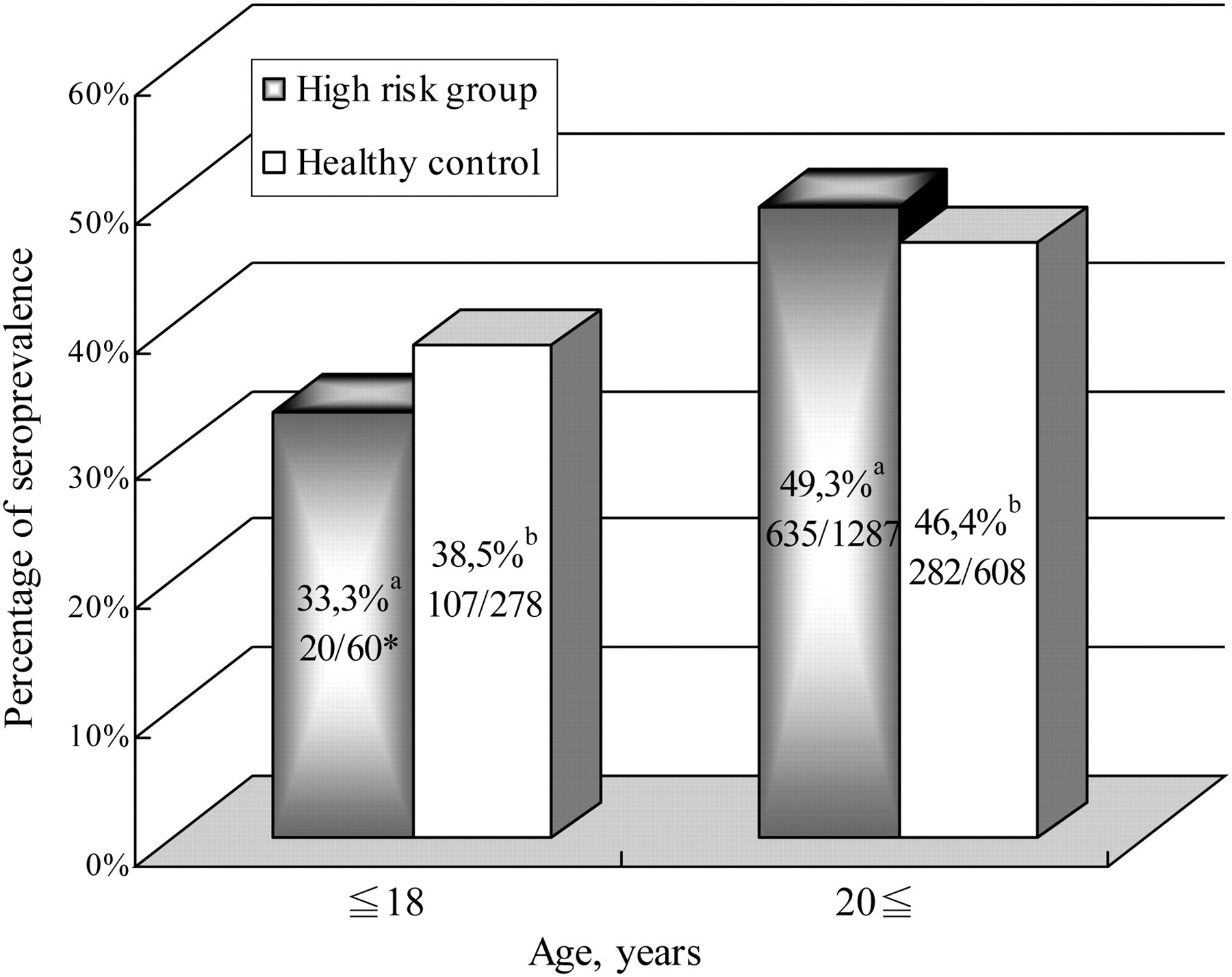
Age-related seroprevalence of hepatitis B surface antibody (HBs Ab). *N–positive for HBs Ab/N–tested. a P < 0.05. b P < 0.05
DISCUSSION
Since 1992 when the first case of HIV-1 infection was reported in Mongolia, the number of reported cases remained low until 2005. However, the number has been increasing sharply since 2005, and 36 cases have been reported as of February 2008 (Ministry of Health, Mongolia, unpublished data). By the estimated report of the Global Fund for AIDS, Tuberculoses and Malaria (‘Impact of AIDS in Mongolia’ 2004), without prevention measures, Mongolian HIV/AIDS prevalence will be doubled every two years and 2500 people will die of AIDS by 2014. Our result supports this estimation. A current prevalence of HIV-1 infection is still low but the risk status of HIV-1 infection must be high because of the very high prevalence of syphilis in FSWs (39.5%), especially in Ulaanbaatar (54.7%). Another report also presented similar prevalence among low-income FSWs in Mongolia (43%). 9 Schwebke et al. 7 reported the prevalence rate (8.6%) of syphilis among 137 male STI clients in Ulaanbaatar in 1998. In our study conducted in 2007, this rate in Ulaanbaatar was 16.5%, suggesting that the prevalence of syphilis is increasing. It is true that these rates were anti-TP. Therefore, it did not mean active syphilis. However, these rates document that the exposure to syphilis is very high. A 100% condom programme is strongly recommended.
According to the unpublished data by NCCD, another risk factor for HIV-1 acquisition is that the predominant route of HIV-1 transmission in Mongolia is through sexual intercourse in MSM. The present study showed higher rates of anti-TP (30%) and anti-HCV (18%) in MSM than those in neighbouring countries: for example, 7% in Beijing (China) and 10% in St Petersburg (Russia) for syphilis and 0.8% or 5.2% in Beijing (China) for HCV. 14–16 These results indicate active high-risk sexual intercourse in Mongolian MSM. There is strong prejudice and discrimination against MSM in Mongolia. Hence, access to the MSM group was very difficult in this study. This barrier makes the delivery of information to MSM difficult. A quick countermeasure to MSM is crucial and a larger serological survey is necessary to grasp the actual prevalence of HIV-1 in Mongolian MSM.
Compared with other STIs, evaluation of hepatitis B was not simple because of the high-prevalence rate in the general population. A hepatitis B vaccination programme has been conducted 18 years ago. Around 35% of people below 18 years have HBs Ab. In contrast, those over 20 years had a significantly higher rate of HBs Ab in both high-risk and healthy control populations. Analysis of HBc-Ab could make it possible to discriminate between HBV-vaccinated and HBV-exposed individuals, which unfortunately we could not perform in this study. This result also suggests the frequent exposure to hepatitis B in Mongolians. Takahashi et al. 10 reported a comparable rate of HBs Ab prevalence, indicating a low selection bias of subjects in this study except for MSM and drug abusers.
The present study demonstrates that HIV prevalence is currently low. However, according to the high prevalence of syphilis and HCV in high-risk populations and the social stigma against MSM, the risk status for HIV-1 infection is estimated to be high. Close monitoring of the HIV epidemic is important in order to take quick measures for the high-risk populations and consequently keep the prevalence of HIV low in Mongolia.
Footnotes
ACKNOWLEDGEMENTS
Dr J Davaalkham is a research fellow of the Japan Foundation of AIDS Research.