
Abstract
The objective of the study was to investigate the HIV-mother-to-child transmission (MTCT) rate in Israel. This was a retrospective study of HIV-infected pregnant women, mainly immigrants from Ethiopia, in six Israeli AIDS centres, in 2000–2005. Medical records of mothers and newborns were evaluated for HIV status, treatment and MTCT rates. Three hundred pregnancies of 241 HIV-infected women, resulting in 304 live births, were studied. In 86/241(36%) women, HIV diagnosis was made during the current pregnancy or shortly after labour. Thirty others were diagnosed during previous pregnancies. Highly active antiretroviral therapy (HAART) was prescribed in 76% of pregnancies. The mean viral load before labour was 23,000 ± 100,000 copies/mL with a mean CD4 of 406 ± 223 (range 4–1277) cells/mm3. Caesarian sections were preformed in 175/300 pregnancies (103/175 with viral load <1000 copies/mL). During labour, azidothymidine (AZT) was given to 80% and nevirapine to 8% of the women. Eighty-eight percent of the neonates received AZT for six weeks. The overall HIV-MTCT rate was 3.6%. MTCT correlated significantly with delayed HIV diagnosis, low CD4, lack of HAART during pregnancy and lack of perinatal treatment. HIV treatment of mothers and their newborns throughout pregnancy, labour and perinatal period are crucial for effective prevention of MTCT, emphasizing the need for early HIV screening, diagnosis and treatment.
Introduction
Mother-to-child transmission of the human immunodeficiency virus (HIV-MTCT) is the cause of most paediatric HIV infections worldwide. It may reach 40% or more without intervention.1–5 In the era of highly active antiretroviral therapy (HAART), HIV-MTCT has been dramatically decreased to less than 2% and virtual elimination of HIV in infants by 2010 has been set as a goal for the European region.6,7 However, in Africa and in other undeveloped countries, HIV vertical transmission is still a major medical problem. 8
HIV vertical transmission can take place in utero, but mostly occurs during delivery or postnatally through breastfeeding. Efforts to reduce HIV vertical transmissions have, therefore, included specific interventions during pregnancy, labour and the postnatal period. 5 HIV-MTCT prevention programmes should include three parts: (1) HAART given to all women regardless of their HIV status during pregnancy as well as treatment during and after labour to all mothers and neonates; (2) Elective caesarean section for specific indications (e.g. viral load >1000 copies/mL); (3) Refraining from breastfeeding.9–11 The implantation of such a programme, including HIV screening during pregnancy for an early diagnosis differs between countries and among populations within the same country.
In Israel, the vast majority of HIV-infected females are immigrant Jews from Africa (Ethiopia). A smaller group immigrated from east Europe, mainly the former USSR. HAART as well as all other medical interventions, including feeding formula for neonates, are available in Israel with no charge for all HIV-infected patients. Therefore, AIDS clinics in Israel are unique for treating African patients with HIV (subtype C) with all western medical facilities.
In the present study, we evaluated 300 pregnancies of HIV-infected women from six Israeli AIDS centres, in the HAART era (2000–2005). Our objectives were to determine the MTCT rate among our patients (mainly Ethiopian immigrants), the predictors for HIV vertical transmission and the implantation of the HIV-MTCT prevention programme in Israel.
Methods
Study participants
From January 2000 to October 2005 all HIV-infected pregnant women and their infants in six Israeli AIDS centres were retrospectively evaluated. Mothers’ files were studied for mode and time of HIV diagnosis, HIV status during pregnancy and labour, treatment during pregnancy, mode of delivery and MTCT rates. Infants’ files were evaluated for postpartum therapy, breastfeeding and outcome.
Procedures
Plasma HIV viral load was determined by a commercial kit (COBAS Ampliprep/Amplicor version 1.5, standard format; Roche Molecular System, Branchburg, NJ, USA). Infants’ cellular HIV-1 DNA was quantitated by home-made polymerase chain reaction (Central Virology Laboratory, Public Health Services, Ministry of Health, Sheba Medical Center, Tel Hashomer, Israel). All infants were evaluated at day 2 and thereafter at months 1 and 4. HIV– enzyme-linked immunosorbent assay testing was performed at the age of 18 months.
CD4 cells were counted by fluorescence activated cell sorting using fluorescein isothiocynate CD4 monoclonal Abs (IQ Products, Groningen, The Netherlands).
Statistical analysis
For uni-variables comparison we used the Student's t-test for quantitative variables, and the chi-square test or Fisher's exact test for qualitative variables. Data are presented as mean ± standard deviation. P ≤ 0.05 was considered significant.
Results
Mothers’ characteristics
Demographic characteristics of 241 HIV-infected pregnant women
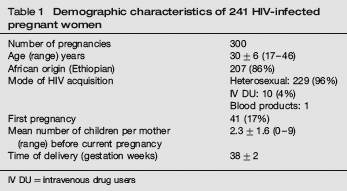
IV DU = intravenous drug users
Treatment during pregnancy and maternal adverse events
HAART was prescribed in 229 (76%) of 300 pregnancies. In 100 pregnancies therapy was required only for MTCT prevention and was stopped after delivery. Treatment with HAART was recommended to 197/229 (86%), with dual therapy (azidothymidine [AZT] and lamivudin) to 20/229 (9%) and with monotherapy (AZT alone) to 12/229 (5%). Severe adverse events related to ART (requiring hospitalization or change in protocol) were documented in 14 (6%) of all treated women. Adverse events included diarrhoea (six cases), anaemia related to AZT (three cases), diabetes mellitus (two cases), nevirapine-associated rash (one case), Steven-Jhonson syndrome (one case) and liver function tests disturbances (two cases). All events were resolved with drug change and no deaths were reported. In 71 (24%) pregnancies no antiretroviral (ARV) were prescribed because of late diagnosis, lack of compliance or patients refusal. In all 45/71 (63%) of these women were diagnosed with HIV during or after current pregnancy (16 of them during labour).
The mean HIV-viral load before labour in the entire cohort was 23,000±100,000 copies/mL (Log 4.3±5; range: <400– 10 6 ). In 162 pregnancies, viral load was below level of detection (<400 copies/mL). Undetectable viral loads were more common, though not statistically significant, among patients who were treated with HAART rather than with mono or dual therapy (142/197 (72%) versus 20/32 (62%); respectively). The mean CD4 count before labour was 406±223 (range 4–1277) cells/mm3. In 42 pregnancies, the CD4 count was below <200 cells/mm3.
Mode, time of delivery and treatment during labour
The median time of delivery was 38±2.2 (range 24–42) weeks of gestation. Nineteen (6.3%) pregnancies ended prematurely (weeks 24–35). During labour, AZT (IV) was given to 242 (80%) of our pregnant women and an additional single dose of nevirapine to 25 (8%). Caesarian sections (electives and non-electives) were performed in 175 (58%) of 300 pregnancies, HIV viral load below 1000 copies/mL was observed in 103 (59%) of them. Only minor postoperative complications such as minor wound infection and minor bleeding were documented. One hundred and twenty-five (42%) deliveries were vaginal, HIV viral load was below 1000 copies/mL in 74 (59%) of them.
Neonatal treatment and outcome
The 300 pregnancies reported here, resulted in 304 live births and two still births. Of 304 neonates 269 (88%) received AZT for six weeks and 48 (16%) received an additional single dose of nevirapine. As many as 16 (5.3%) neonates were breastfeed. In our cohort, 37 (12%) neonates required treatment in the neonatal intensive care unit. Perinatal deaths (still births and deaths within the first 28 days of live) were documented in six (2%) neonates, and three (1%) other infants had died within the first eight months of life (only one of them was infected with HIV). Fifteen (5%) babies were born with birth defects, six cardiac, two neurological, one congenital diaphragmatic hernia and six others.
HIV-MTCT rate
The rate of HIV-MTCT in the entire cohort was 3.6% (11 out of 300 pregnancies). Eight infected infants were born to mothers of African origin. Vertical transmission decreased from 10 of 162 pregnancies between the years 2000–2002 (MTCT rate of 6.1%) to one of 138 pregnancies in 2003–2005 (MTCT rate of 0.7%; P = 0.01). HIV-MTCT rate correlated with the time of HIV diagnosis of the mothers. Thus, HIV vertical transmission was observed in 9.3% (8/86) of women diagnosed with HIV during current pregnancy/labour compared with 1.4% (3/214) of transmission in women diagnosed with HIV in the prepregnancy period (P = 0.0009).
Characteristics of mothers and infants, according to HIV-MTCT status
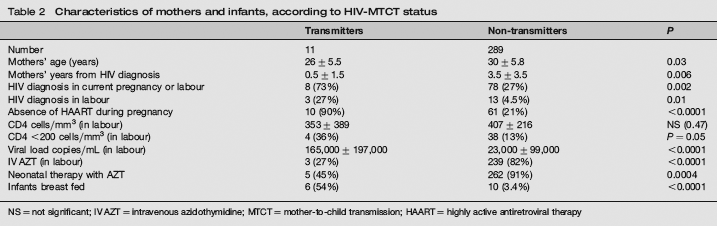
NS = not significant; IV AZT = intravenous azidothymidine; MTCT = mother-to-child transmission; HAART = highly active antiretroviral therapy
HIV-MTCT and mode of delivery
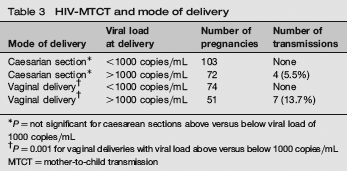
P= not significant for caesarean sections above versus below viral load of 1000 copies/mL
P = 0.001 for vaginal deliveries with viral load above versus below 1000copies/mL MTCT= mother-to-child transmission
Discussion
The implantation of HIV-MTCT prevention programme in Israel is quiet effective since a relative low rate (3.6%) of HIV-MTCT was observed in our cohort. Moreover, the rate of HIV-MTCT has dramatically decreased (to 0.7%) in the last three years of our retrospective study. Early HIV diagnosis is a prerequisite for the application of all interventions to reduce HIV-MTCT. Therefore, it is a crucial component of any prevention programme. In our study as much as 48% of the women were diagnosed with HIV during pregnancy. Moreover, three of 11 children were vertically infected by women who were not diagnosed with HIV before delivery, emphasizing the importance of antenatal testing even in a country with a low HIV prevalence like Israel. Routine voluntary HIV-antibody testing of pregnant women on an opting-out basis, regardless of risk factors or ethnic origin, has been recommended by most guidelines and was implanted by many countries with a high acceptance rate.12,13 We believe that offering HIV-antibody testing to all pregnant women in Israel will enable us to identify all infected women during early stages or pregnancy without stigmatizing women of high-risk groups.
Numerous other risk factors for HIV-MTCT have been documented in the past,11,13,14 and several different interventions to prevent HIV-MTCT have been suggested with efficacy demonstrated for HAART prophylaxis, avoidance of breastfeeding and elective caesarean section. 14 In our cohort, the absence of any ART during pregnancy, high HIV viral load and severe immune deficiency in labour correlated with HIV-MTCT, whereas the treatment of mothers with intravenous AZT during labour and of neonates with syrup AZT for the first six weeks of life negatively correlated with HIV-MTCT (Table 2). Although the differences in transmission rates between women treated during pregnancy with HAART and those treated with mono or dual therapy were not statistically significant, in the HAART era, combination therapy with HAART (as opposed to mono or dual therapy) should be offered to all HIV-infected pregnant women regardless of their viral load or CD4 counts.
Breastfeeding is associated with an approximate doubling of the HIV-MTCT risk. 13 Indeed in our study, breastfeeding highly correlated (P = 0.0001) with HIV-MTCT rate (Table 2). Since infant formula is available to all infants of HIV-infected mothers in Israel, avoidance of breastfeeding is highly recommended.
The preferred mode of delivery for HIV-infected pregnant women in the HAART era has been an issue of debate.13,15,16 In the European mode of delivery randomized trial the HIV-MTCT rate among women allocated to vaginal delivery was 10.5% versus 1.8% in the elective caesarean section group. 15 Similar results were reported in a large meta-analysis involving 15 American and European observational studies. 13,16 However, the added benefit of elective caesarean section on reducing HIV-MTCT in women with low plasma HIV viral load (<1000 copies/mL) treated with HAART is uncertain. 13 In our study, vaginal delivery for women with a viral load of more than 1000 copies/mL correlated with higher rates of HIV-MTCT as compared with caesarean section deliveries (Table 3). For those women, elective caesarean section should be recommended. Among women with a HIV viral load of less than 1000 copies/mL no vertical transmission was documented in our study regardless of mode of delivery (Table 3). For the latter women there is no proven benefit for caesarean section, thus vaginal delivery should be considered.
Although the vast majority of infants born to HIV-infected mothers in the HAART era are protected from vertical transmission, they are exposed to ARV drugs, for which there is only limited information on neonatal toxicity. In our study, 37 of 304 (12.2%) newborns to HIV-infected women (24 of these infants were exposed to HAART during pregnancy) required treatment in the neonatal intensive care unit, this is higher than the rate for non-HIV deliveries in Israel, which is about 8%. 17 Further studies are needed to define the prevalence and risk factors of neonatal morbidity in the HAART era.
In conclusion, implantation of HIV-MTCT prevention programme in six Israeli centres was successful and a low rate (0.7%) of vertical transmission was observed in the last three years of our study. Nevertheless, an early screening and diagnosis of HIV-infected pregnant women remains a major goal for our HIV-MTCT prevention programme in order to improve antenatal care, and to further decrease HIV transmission.