
Abstract
The prevalence rate of lower gastrointestinal bleeding in patients with AIDS is around 2.6%. A 42-year-old woman with AIDS (CD4 count 9/μL) and recently treated for disseminated histoplasmosis presented to the emergency room with melena, severe anaemia and fever. A colonoscopy showed an umbilicated colonic nodule mimicking a carcinoma of the colon. The biopsy showed intracytoplasmic microorganisms compatible with Histoplasma capsulatum. She had poor compliance to the itraconazole when discharge on previous admission. Despite the fact that colonic histoplasmosis is uncommon, the mortality rate is around 8% and clinicians should be aware of the clinical presentation of histoplasmosis when recur, especially in patients not taking the itraconazole for long-term treatment.
Keywords
INTRODUCTION
Histoplasmosis, caused by Histoplasma capsulatum var capsulatum, is the most prevalent endemic mycosis in the United States. While most infections are asymptomatic or self-limited, immunosuppressed patients may develop acute pulmonary infection or severe and progressive disseminated disease. In patients with AIDS, who reside in endemic areas and who are not receiving antiretroviral therapy, the risk of histoplasmosis is 2–5%. 1 Dissemination of the infection is a severe opportunistic infection with poor prognosis when left untreated among patients with AIDS, 2 and it is more common in patients with a CD4 count ≤150 cells/μL.
We report here a middle aged patient with advanced AIDS stage (CD4 = 9/μL) with recurrent histoplasmosis presenting with a lower gastrointestinal (GI) bleeding from a lesion mimicking a carcinoma of the colon. We emphasize the continuous use of itraconazole as prophylaxis.
CASE REPORT
A 42-year-old HIV-infected black woman with CD4 = 9/μL, in AIDS, presented with the complaint of dark stools (melena), weakness, shortness of breath, chest pain and significant weight loss for the last two weeks. The patient denied any abdominal pain, palpitations or dizziness. She had a history of untreated hepatitis C, hypertension, cocaine abuse, congestive heart failure and AIDS. She was diagnosed with disseminated histoplasmosis one month ago. Nonetheless, she stated that she had not been taking the prescribed itraconazole. A poor compliance was also noted to the antiretrovirals. Other medications included carvedilol, furosemide, weekly azithromycin and daily co-trimoxazole. Her temperature was 101ºF, blood pressure 120/63 mmHg with no orthostatic drop, heart rate 88/minute. On examination, the conjunctiva was pale. Submandibular nodes were palpable. Heart sounds were regular, a 2/6 systolic murmur was audible in the precordial area. The rest of the examination was unremarkable. Electrocardiogram and chest X-ray were normal. Upon arrival her haemoglobin was 6.6 g/dL, haematocrit 20%, mean corpuscular volume 80.8 fl, iron 17 µ/dL (30–160), TIBC 305 µ/dL (228–428), ferritin 153 ng/mL (5–204), transferrin saturation 6%, lactate dehydrogenase 282 U/L (98–192), white cell count (diff) 3500 cells/mm3 (neutrophils 46%; lymphocytes 33%; eosinophils 11%; monocytes 9%), platelet count 234,000/mm3, CD4 count 9/μL. Occult blood was positive. Urine cultures and blood cultures including for fungi and mycobacteria were negative. Cryptococcal serum antigen and rapid plasma reagin were negative. Co-trimoxazole, azithromycin prophylaxis and itraconazole were started. Because of her significant symptomatic anaemia, she received five units of packed red blood cells. An upper GI endoscopy was performed for assessment of her melena, but no lesions were found. Then, a colonoscopy showed an oozing umbilicated nodule at 40 cm from the anus (Figure 1). The biopsy showed no malignant lesion but intracytoplasmic microorganisms compatible with H. capsulatum. Immunochemistry for cytomegalovirus (CMV) antigen resulted negative. Induction treatment with amphotericin B was started, and continued with oral itraconazole upon discharge. Haemoglobin on discharge was 10.2 g/dL. Six months later, the patient was asymptomatic.
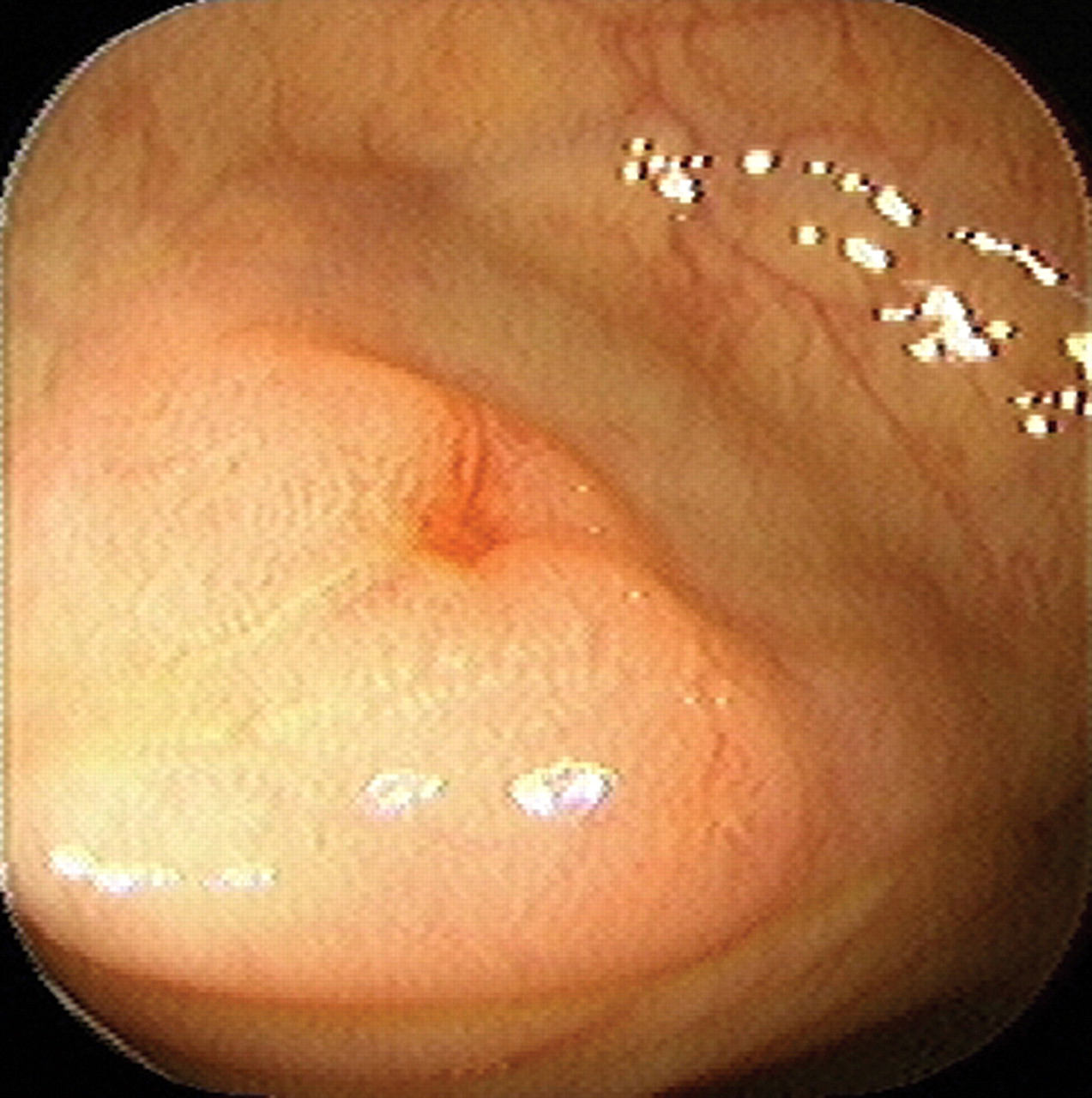
Umbilicated nodule 40 cm distance from the anus, with a small amount of blood oozing from the lesion. The biopsy showed intracytoplasmic microorganisms compatible with Histoplasma capsulatum
DISCUSSION
We report a case of advanced AIDS stage with low CD4 that presented with melena and symptomatic severe anaemia caused by H. capsulatum presenting as a haemorrhagic colonic nodule. The patient was successfully treated and discharged asymptomatic.
The prevalence of lower GI bleeding in AIDS patients is 2.6% and the most common cause is CMV infection. 3 Other causes include herpes virus, histoplasmosis, bacillary angiomatosis, Kaposi's sarcoma and lymphoma. Despite the fact that histoplamosis may occasionally present as lower GI bleeding with melena, it may carry a high mortality rate. In addition, out of 52 gastrointestinal histoplasmosis (GIH) patients with AIDS, four died from GI bleeding (7.6%). 4 Histoplasmosis is not a benign infection in AIDS. It tends to disseminate in almost 95% of AIDS patients. 5 The overall incidence of this morbid association is 2.9–20%. 6,7 The GI tract is affected in 3–12% of patients and bleeding is the clinical presentation in 33% of them; however, colon is the organ most frequently compromised (67%). In another series, out of 18 patients, only one presented endoscopic findings similar to our patient. 8 Furthermore, colonic masses mimicking carcinoma have been described in case reports, 9 case series 10 and review articles. 11
Moreover, GIH is more likely among severely immunocompromised patients with AIDS not receiving highly active antiretroviral therapy. Typical manifestations include diarrhoea, fever, abdominal pain, and weight loss. Diagnosis is confirmed by blood or GI tissue culture or biopsy. Improvements in antiretroviral and antifungal therapies appear to have reduced the incidence of GIH and may improve the prognosis of this disease. Future studies are warranted.
In summary, lower GI bleeding is infrequent in patients with AIDS, but when it happens it is usually caused by opportunistic diseases specifically related to immunodeficiency. Although some of these conditions are potentially treatable medically, in-hospital mortality is high and long-term prognosis is poor because of AIDS-related co-morbidity. Patients with HIV infection who present with GI symptoms should be fully evaluated because of the increasing number of associated diseases that display similar clinical and endoscopic findings. In conclusion, GI involvement of disseminated histoplasmosis should be considered in the investigation of AIDS patients with melena in the setting of a previous episode of histoplasmosis in the past.