
Abstract

These excellent case reports presented by Dr O'Mahony et al. 1 and Dr Annan and Dr Boag 2 raise important clinical and therapeutic issues with regards to dual infection with N. gonorrhoeae (Ng) and C. trachomatis (Ct). The reports afford an opportunity to consider a potential therapeutic dilemma in the management of proven or potential, severe combined infection with Ct and Ng. Does the following hypothesis merit consideration and debate?
Will the effective treatment for severe infections with Ng inevitably lead to ‘inadvertent’ suboptimal therapeutic management of Ct?
Drs Annan and Boag identify gonococcal ophthalmia and periorbital cellulitis in a HIV-positive man without genital infection. 2 This man was stabilized on antiretroviral therapy with CD4 count of 736 cells/mm and viral load <50 RNA copies/mL. The authors prescribe i.m. therapy with ceftriaxone 1 g o.d. for 10 days. Reference is also made to treatment with ‘a weeks’ course of doxycycline to cover the possibility of concomitant infection with Chlamydia trachomatis'.
While it is noted that genital samples were negative, topical chloramphenicol may decrease the diagnostic reliability of conjunctival sampling for Ct. The risk of permanent visual impairment with either or both of these pathogens is well-recognized. American Ophthalmologists referring to ocular viral and bacterial infections would consider that ‘only cases with extremely pathogenic organisms such as Chlamydia trachomatis or Neisseria gonorrhoeae are expected to develop complications.’ 3
Oral antichlamydial therapy may be recommended for as long as three weeks 3 to minimize or avoid such complications in ophthalmic practice. However, infections with the same ‘extremely aggressive pathogen’ in the genital tract would usually be treated for only one or two weeks, or even stat doses of azithromycin 1 g should the infection be considered ‘uncomplicated’.
The aggressive nature of chlamydial eye disease would appear to be visible in Figure 1 2 where there is apparent evidence of early, marginal neo-vascularization of the cornea (04:00–07:00 hours). Might these features potentially be associated with early calcification? Residual corneal scarring of keratitis is recorded in this case report. 2
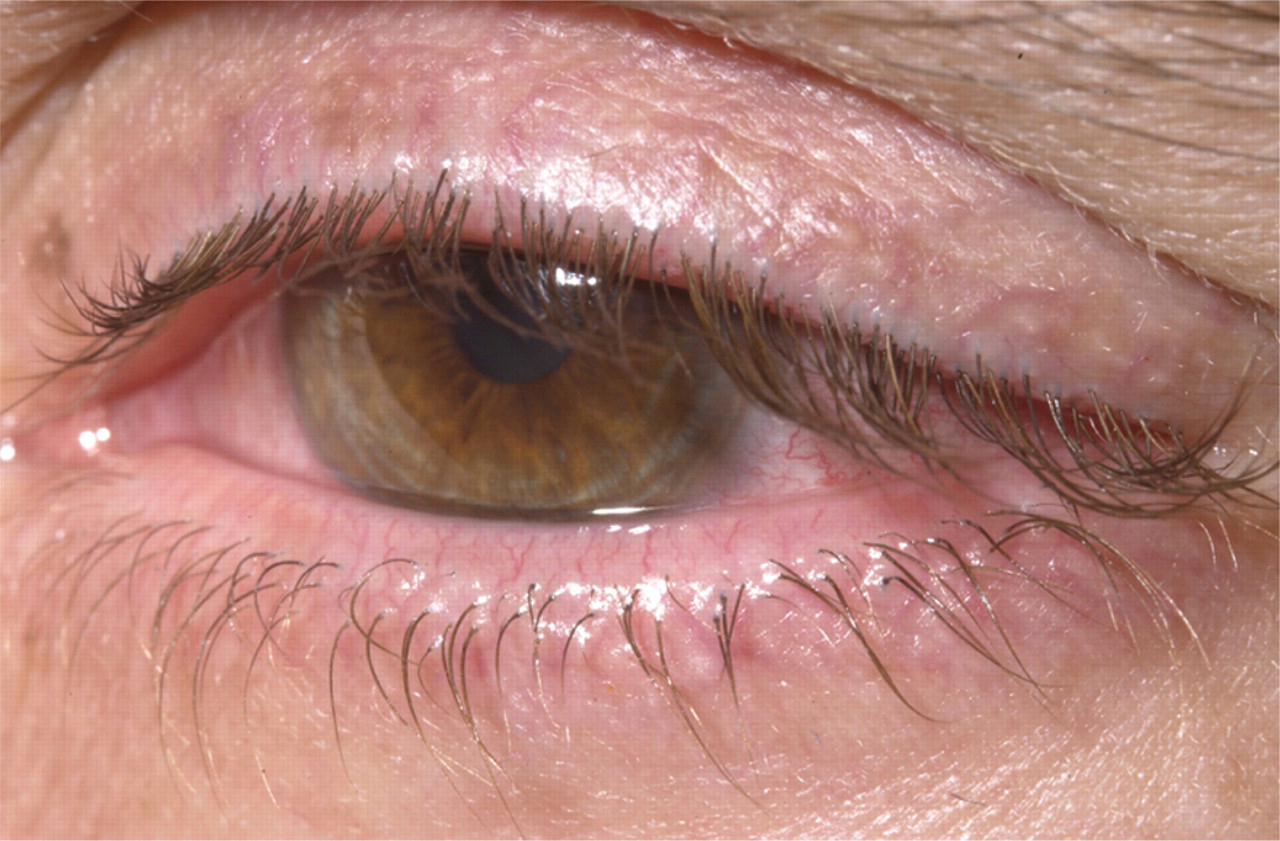
Ocular appearance after 10 days' treatment with ceftriaxone 1 g i.m. daily. However, there was residual corneal scarring. With thanks to Dr N T Annan for supplying the photograph
In considering broader issues of clinical management, should this man be advised that future/continued use of contact lenses be avoided?
In this patient, gonococcal kerato-conjunctivitis was clearly anticipated, identified and intensively managed. Additional clinical features appear to be present. Photophobia might be anticipated. A palpable increase in the preauricular node may have supported C. trachomatis co-infection (or concomitant viral infection).
No reference is made to the presence or absence of lymphoid follicles in the fornices. In chlamydial eye infections, ‘follicular hypertrophy is observed when the infection has been present for more than one week. The follicles are usually predominantly in the upper and lower fornices and take on a more solidly infiltrated and fleshy appearance if the infection has persisted for several weeks or months. Occasionally a fine epithelial punctate keratitis may develop. The keratitis usually develops 2–3 weeks after the onset of conjunctivitis.’ 4
The cautious use of concomitant doxycycline therapy to cover possible chlamydial co-infection is noted. However, ceftriaxone 1 g daily for 10 days may adversely affect antichlamydial therapy.
Patients with Ng and Ct co-infection or patients with disseminated Ct infection have often received beta-lactam antibiotics prior to, or during antichlamydial therapy. It is therefore hypothesized that effective treatment for one dangerous pathogen (Ng) might create a therapeutic environment in which it is much more difficult to treat and eradicate Ct.
Ct can be interrupted in its lifecycle (aberrant phase) resulting in extended replication time or persistent states. Even with nucleic acid amplification testing, exposure to non-chlamydial anti-microbial regimens could lead to ‘false-negative’ Ct investigation. 5 The Ct plasmid is believed to be retained during persistence. However, any change in the plasmid that results from intercurrent (non-antichlamydial) antibiotics would be expected to decrease the diagnostic efficacy of nucleic acid-based diagnostic systems that target the plasmid. Strand displacement amplification (SDA) testing is plasmid-dependent. Transcription mediated amplification (TMA) is non-plasmid-dependent. In addressing the entire range of nucleic acid-based test systems – in the absence of hard data – some experts would assume that we would still fail to diagnose many persistent state infections.
With reference to induced persistent states of Ct, we expect that the amount of ompA, the gene encoding the major outer membrane protein (MOMP) in antibiotic-induced persistent states is similar to that in normal chlamydial organisms. Therefore, any nucleic acid-based assay that detects the ompA gene should stand a chance of identifying these organisms. However, the overall organism burden is much lower (as shown in animal models) and is more likely to be in less easily accessed tissue (e.g. the endometrium), so detection is hampered by these features.
In summary – on occasion, failure to diagnose persistent infections will occur despite great improvements in sensitivity compared with historical diagnostic tools.
Is discussion of induced persistent states of Ct relevant in the case of the 17-year-old female with complex pelvic abscess reported by Dr O'Mahony et al. 1 Here, it is possible that when ‘asymptomatic’ chlamydia infection was identified in the local contraception clinic, endometrial involvement may have already developed. Intercurrent use of beta-lactam antibiotics (not identified) and/or use of stat azithromycin might have induced a persistent state of chlamydia within the endometrium, with potential reactivation following surgical instrumentation. 6
The presentation of these two comprehensive case history reports is appreciated. In addition to hypothetical issues of adverse therapeutic interaction in such patients, genitourinary physicians are reminded of the importance of working in close collaboration with our colleagues in ophthalmology and gynaecology.