
Abstract
We undertook this study to try to determine whether disease outcomes were poorer in patients with HIV infection whose general practitioner (GP) was unaware of their status compared with those whose GP was aware. The notes of 375 HIV-positive patients attending Edinburgh's genitourinary (GU) medicine clinic were reviewed. The GPs of 292 patients (78%) had been informed of their patient's HIV infection. Advancing disease was associated with disclosure of the status to GPs (P = 0.037) but no significant association was found between informing GPs and the viral load results of treated (P = 0.389) and untreated patients (P = 0.070). Twenty-three percent of patients had had one or more bacterial sexually transmitted infections (STIs) while receiving their HIV care at a GU medicine clinic. Patients diagnosed with an STI were less likely to disclose their HIV status to their GP (P < 0.0005). Nondisclosure of the HIV status to a GP may be a predictor of unsafe sexual practices.
Keywords
Introduction
HIV infection is unusual in that it is not automatic for general practitioners (GPs) to be informed of a patient's diagnosis. Many patients undergo HIV testing and thus discover their status at anonymous settings such as genitourinary (GU) medicine clinics. Good clinical practice and national guidance expects that the patient's GP should be informed of a diagnosis of HIV infection, but UK audits consistently show a percentage of cases in which this does not occur.1,2 Reasons for this include concerns about confidentiality, lack of HIV knowledge or expertise, or simply failing to register with a GP. This is disappointing as HIV is a complex, chronic condition affected by and impinging upon many aspects of a patient's daily life, and GPs are much better placed than hospital-based services to deliver care in such situations. Treatment goals in HIV medicine are also broadening from control of viral replication and sexual health promotion to include issues such as prevention of cardiovascular disease, a subject in which GPs have much more experience than HIV specialists. They also have access to supporting services like smoking cessation. 3 We undertook this study to try to determine whether there was any detriment to patients, in terms of disease outcomes, if the GP was unaware of their status compared with those whose GP was aware.
Methods
From October to December 2006, the case-notes of all HIV-positive patients attending the Edinburgh GU Medicine Department were reviewed and results from the computerized laboratory system were scrutinized. There were 497 HIV-positive patients registered at the GU medicine clinic. Patients were deemed eligible for inclusion in the study if they had been under care from GU medicine for at least one year and the GU medicine clinic was their only specialist centre for HIV care. Disclosure of an HIV diagnosis was judged according to the presence or absence of written correspondence with the patient's GP. Disease outcomes measured included last CD4+ lymphocyte cell count (cells/mm3), Centres for Disease Control (CDC) HIV disease stage and last viral load (copies/mL) for patients not on antiretroviral therapy (ART). CD4+ cell count was categorized into three groups: counts <200, 200–500 and >500 cells/mm3. CDC stage was recorded as the stage at disclosure for patients whose GP was informed or current CDC stage for patients whose status remains undisclosed. Viral load for patients taking ART was classified as having been consistently undetectable (<50 copies/mL), intermittently detectable or consistently detectable for the past year. Patients with a maximum of two transiently raised viral loads, often referred to as ‘blips’, were regarded as falling into the undetectable group. 4 One patient on structured treatment interruptions, one pregnant woman and nine patients who had started treatment within the last year were excluded from this group. Viral resistance to antiretroviral drugs was assessed from resistance test results, excluding one case of primary resistance. Using a computer-based system of laboratory results running from 1999, cases of syphilis, gonorrhoea or chlamydia were recorded.
Statistics
Categorical variables were tested for association using the chi-squared test of association, except where <80% of the expected frequencies were of value 5 or more when Fisher's exact test was applied. The chi-squared test for linear trend was applied where appropriate. Continuous data were examined for normality using histograms and the Shapiro–Wilks test. The Mann–Whitney U test was used to assess the difference between two medians of non-parametric data. All tests were performed using the Statistical Package for the Social Sciences 14.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Population demographics (n = 375 unless otherwise stated)
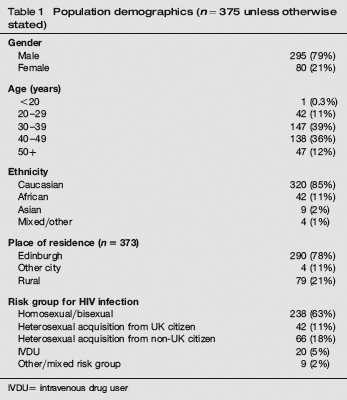
IVDU= intravenous drug user
The GPs of 292 patients (78%) had been informed of their patient's HIV infection. Of these patients, 184 (63%) had informed their GP within six months of diagnosis or transfer to GU medicine. The remainder informed their GP within a range of six months to 20 years. The HIV-positive status of nine patients was disclosed to their GP accidentally. The GU medicine clinic had ceased communication with the GPs of four patients, who had been previously informed of their patient's diagnosis.
Relationship between last CD4+ cell count (cells/mm3) and disclosure

GP = general practitioner
No significant association was found between informing GPs and the viral load results of treated (Fisher's exact test = 2.909; P = 0.700) and untreated patients (U = 1174; P = 0.070).
Relationship between CDC Disease Stage and disclosure

A = asymptomatic; B = minor symptoms; C = major symptoms/AIDS; CDC = Centers for Disease Control; GP = general practitioner
Eighty-five percent of the study population have had no evidence of virological resistance to ART. Of the remainder, 29 had resistance to ART that had been commenced before 1998, 18 to therapy post-1998 and 10 to both. A significantly greater proportion of patients with resistance were shown to have informed their GP of their diagnosis (95%) compared with patients without resistance (75%) (χ2 = 9.976; P = 0.002). This difference was greatest when comparing patients without resistance to those with resistance to ART since 1998 (Fisher's exact test; P = 0.009), in whom poor adherence would be the most likely contributing factor.
Bacterial sexually transmitted infections
Twenty-three percent of patients have had one or more bacterial sexually transmitted infections (STIs) while receiving their HIV care at this GU medicine clinic, of whom 36% had more than one infection. An association between having an STI and not disclosing one's HIV status was apparent (Figure 1) (χ2 = 12.364; P = 0.002). A significant linear relationship was also demonstrated, when the chi-squared test of trend was applied (χ2 = 12.313; P < 0.0005).
Relationship between disclosure and STI status (n = 373)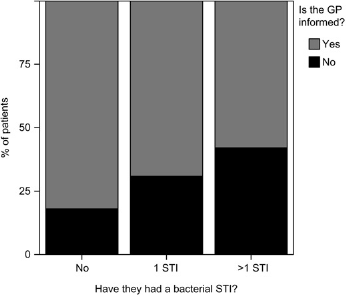
Discussion
Our hypothesis was that patients who declined GP involvement in their HIV care would take ART less effectively leading to the increased risk of treatment failure, viral resistance and low CD4 count. There was however, the potential for confounding between variables; for example it was demonstrated that taking ART was independently associated with significantly higher disclosure rates (χ2 = 34.287; P < 0.0005) and these are the patients who are more likely to have advanced disease. A study of HIV-positive women in London has also showed that symptomatic patients were more likely to inform their GP. 5
Rates of non-disclosure were higher in patients with counts between 200 and 500, compared with those with counts above 500 or below 200 (Table 2). This apparent anomaly may be explained when one considers typical clinical situations; patients with counts above 500 are more likely to be taking ART, therefore more likely to disclose to their GP and those with counts under 200 are more likely to have advanced CDC stage again predicting disclosure.
Advancing disease stage was associated with increasing disclosure (Table 3). Because the disease stage was recorded at the time of disclosure we can assume that this association does not arise because the act of informing the GP leads to poorer health outcomes.
Resistance to ART taken before 1998 may have occurred because of inappropriate drug combinations, inefficient drugs and clinical inexperience. After 1998 and the introduction of highly active antiretroviral therapy, resistance would have been more likely to occur due to poor adherence. It might therefore be predicted that patients who did not inform their GP would have higher rates of resistance, and consequent treatment failure with ART post-1998. The reverse was actually demonstrated and may simply reflect higher levels of viral resistance in patients taking ART for many years, and who are thus independently more likely to inform their GP.
There was, however, an unexpected association between non-disclosure and poor sexual health, as reflected in the increased diagnosis of acute bacterial STIs. This is an important observation, as clearly there is a potential for ongoing transmission of HIV to sexual partners. Possible explanations for this association include denial of HIV infection, fatalistic attitudes, poor self-esteem and an inability to engage with health services. STI results were only available from 1999; therefore, data for patients registered pre-1999 were unreliable. Patients could have had STIs treated elsewhere, but there is no other GU medicine service in Lothian.
Health professionals caring for HIV-positive patients need to be aware that non-disclosure of the HIV status to a GP may be a predictor for unsafe sexual practices. Intervention to increase the likelihood of safer sex may be indicated for such patients. We continue to advise all our HIV-positive patients to allow notification of their status to their GP.