
Abstract
The frequency of spontaneous genital arousal (GA) and persistent genital arousal disorder (PGAD) in women is unknown. The aim of this study was to conduct an anonymous survey to assess the frequency and nature of spontaneous GA and PGAD in women attending a walk-in sexual health clinic in London. Female patients completed a questionnaire, which included demographic information, medical, psychiatric and gynaecology history, the hospital anxiety and depression scale, and a somatization scale. Patients were then asked to complete three questions regarding spontaneous and persistent GA. Any patient with one or more symptoms then answered questions about the distress, intensity and duration of sensations. Ninety-six subjects participated. The mean age was 28.97 years. Thirty-two women (33.3%) answered ‘yes’ to at least one question regarding spontaneous or persistent GA and six women (6.3%) women answered ‘yes’ to all three questions. Only one subject fulfilled all five diagnostic criteria for PGAD. In conclusion, women report a high rate of spontaneous GA in the absence of desire or excitement. This has not been well described previously. A small proportion of women report multiple features of spontaneous and persistent GA, with chronicity over years, but without distress in most cases. Larger studies are needed.
INTRODUCTION
Female sexual problems are common, with sexual desire and sexual pain problems being the most prevalent. 1,2 A relatively new complaint has received some attention in recent years, namely that of persistent genital arousal (GA). In this condition, spontaneous GA occurs and persists in the absence of any conscious sexual desire or interest. 3 Previously known as persistent sexual arousal syndrome, persistent genital arousal disorder (PGAD) is now emerging as an area of interest in sexual medicine. Provisional data, predominantly observational and descriptive, have begun to shape our basic understanding of the condition. There remain, however, many unanswered epidemiological and clinical questions, not least its prevalence and associated distress. 3–5
PGAD is characterized by unprovoked GA in the absence of sexual desire. Suggested diagnostic criteria for PGAD include involuntary persistent genital and clitoral arousal, GA unrelieved with orgasm, GA unrelated to sexual desire, and GA that is intrusive or unwanted, and at least moderately distressing. 3 The duration of ‘persistence’ has not yet been clearly defined. PGAD is diagnosed if all five of the criteria are reported.
Research has shown that some women do not meet all the five criteria needed for a diagnosis of PGAD, but do report some of the features, and appear to experience more intermittent and less distressing spontaneous GA. Indeed some women find these GA sensations reassuring and endorse words such as ‘sexy, desirable, pleased and youthful’ when asked to describe their reactions. 6
The aetiology of the disorder remains unknown, and to date no studies have successfully identified a definitive cause or precipitating factor. However, organic and psychological associations have been described, furthering speculation that we may be observing a spectrum of physiological and pathological processes. A large online survey provided descriptive data of women who reported all, as opposed to some, of the five features of PGAD. Women who met all criteria displayed higher rates of anxiety and obsessive-compulsive symptoms than those who did not. 6
Case studies have also reported cases of PGAD associated with the cessation of anti-depressant treatment, contrasting with the reduced sexual arousal previously reported with depression or the medications used to treat it. 7 Other reports have suggested that PGAD may be associated with the sleep cycle, ingestion of soy products and cardiac malformations. 8–10
Persistent GA, whether experienced as neutral or as welcome, is considered to be rare. To our knowledge, no studies have investigated how frequently GA sensations, which comprise the PGAD diagnostic criteria, are experienced by women.
Aim of the study
The aim was to conduct a non-interventional survey to assess the frequency and nature of PGAD and GA symptoms in a population of women over 18 years, attending a walk-in sexual health clinic in London.
METHODS
Ethical approval was attained via the National Research Ethics Service, including provisions of Site-Specific Assessment and local Research and Development approval. The study took place during February 2008 within a sexual health walk-in service at St Mary's Hospital, a large clinic in Central London. The majority of patients who attend this clinic are young and attend to have screening tests for sexually transmitted infections (STIs), including HIV. Up to 50% of attendees are asymptomatic. Female subjects over 18 years of age and capable of providing written informed consent were eligible to participate. Subjects were excluded if they did not meet these criteria or if they were not proficient in written English.
A non-validated questionnaire adapted from the original on-line survey was designed and approved, which included sections on demographic information (age, sexuality and marital status), medical, psychiatric (including depression, anxiety, eating disorder, attempted suicide, personality disorder and schizophrenia) and gynaecological history (including PCOS, endometriosis, prolapse, hysterectomy, removal of ovaries or tubes), a medication inventory (past and present, by category), a history of sexual assault, the hospital anxiety and depression scale and a somatization scale. Clinical interviews and assessment of mental state in order to diagnose anxiety or depression were beyond the ethical and practical limitations of this anonymous study.
Patients were then asked to answer three statements regarding GA, which form part of the diagnostic criteria for PGAD (see Figure 1). Any patient with one or more symptoms of persistent GA was then asked to complete more detailed questions about features of PGAD, including distress, intensity and duration (see Figure 2). Completed questionnaires were deposited in a collection box. No identifying demographic or clinical details from the hospital notes were present on the questionnaire, ensuring that subjects could not be identified or linked to their medical notes (a recommendation from the ethics committee). Data were analysed using Statistical Program for Social Sciences software (version 15.0, Chicago, IL, USA). P values of <0.05 were considered significant.

Screening questions for spontaneous or persistent genital arousal
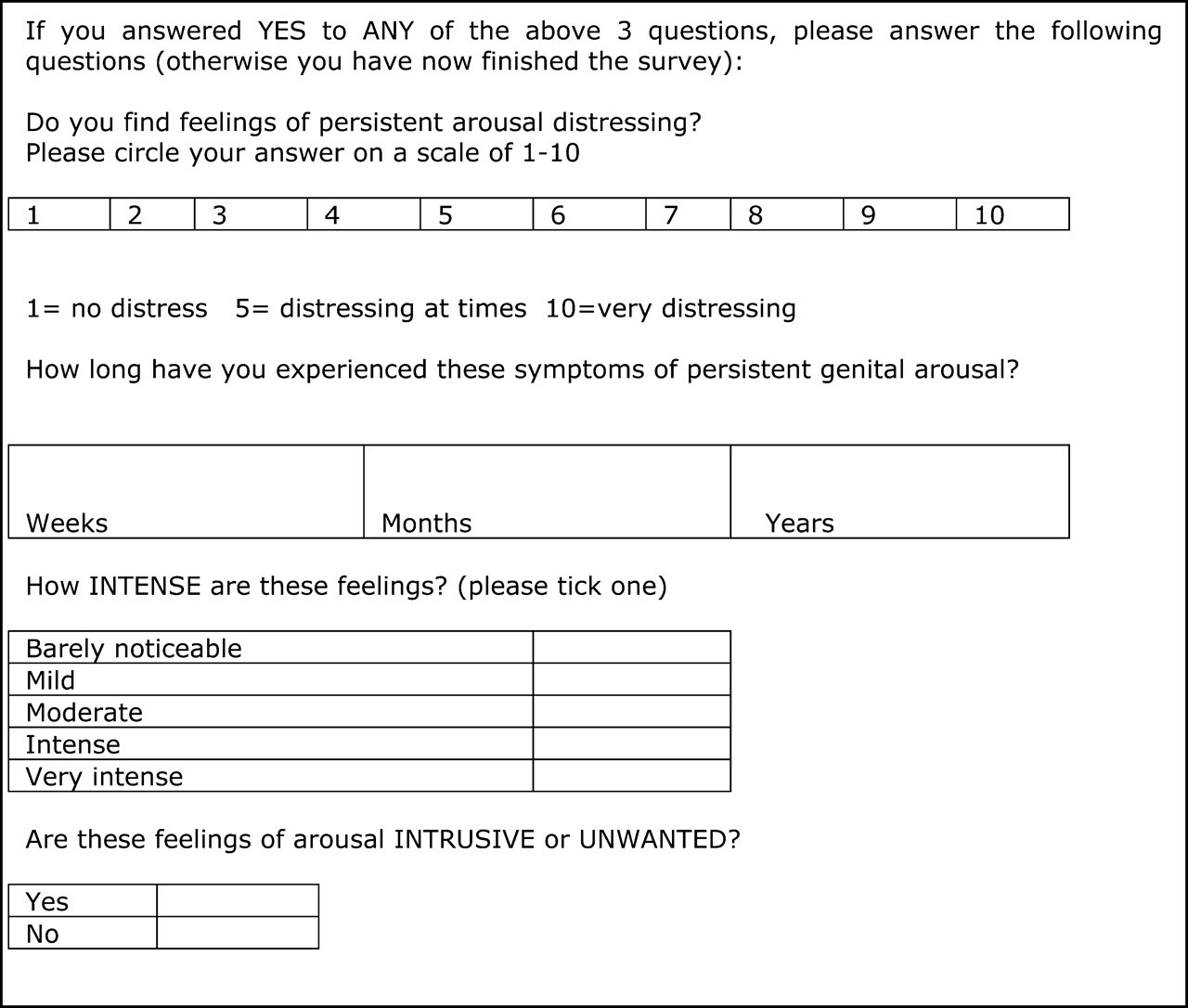
Questions to identify diagnostic criteria of persistent genital arousal disorder
RESULTS
A total of 153 female patients over 18 years of age were invited to enter the study. In all, 96/153 agreed to participate and gave informed consent, providing a response rate of 63%. The median age was 28 years (range 18–64, standard deviation [SD] 7.88). Ninety-one (94.8%) described their sexual orientation as heterosexual and 75% of women were educated beyond 18 years of age. Forty-three (44.8%) were single and 47 (49%) had a regular partner.
Spontaneous and persistent genital arousal
In all, 32/96 women (33.3%) answered ‘yes’ to at least one GA statement (see Table 1). Different combinations of features were reported. In all, 19/96 (19.8%) women had experienced spontaneous GA unrelated to sexual excitement or desire. These women did not report any other feature of the PGAD disorder and were not distressed.
Response to questions on spontaneous and persistent genital arousal (GA)
PGAD = persistent genital arousal disorder
Persistent genital arousal disorder (PGAD)
One subject (1%) fulfilled all five diagnostic criteria for PGAD. This patient was a 38-year-old woman, heterosexual, single and with a high education level. She had a history of depression, anxiety with panic attacks, irritable bowel syndrome and anaemia. She had received antidepressants, antianxiolytics and the combined oral contraceptive pill in the past, but was receiving no medication currently. She had a history of sexual assault. Her total HADS score was 22 (versus study mean 12, SD 7, range 3–31) and her somatization score was 69 (versus study mean 47, SD 15, range 26–101). Reported symptoms of PGAD included intense persistent swelling of the genitals and nipple erection, which was associated with distress measuring 10 on a 10-point scale. Symptoms had been occurring for several years. She had not previously disclosed these sensations to anyone.
Multiple features of persistent GA, without PGAD
Two subjects (2%) reported four of the five diagnostic PGAD criteria, but the associated distress caused by these symptoms was only rated as 4/10 by both women. These women were aged 32 and 20 years, respectively. Both were single, heterosexual and educated beyond 18 years. Total HADS scores were 16 and 9 (study mean 12) and somatization scores were 47 and 71, respectively (study mean 47). One woman had multiple medical disorders, including hypertension, endometriosis and mild asthma, plus a history of depression, anxiety, eating disorder and past overdose. She had previously received the combined oral contraceptive pill (which coincided with the onset of these symptoms). The other woman had no medical or gynaecological history and had previously received the combined contraceptive pill. A mixture of positive and negative emotions was evoked regarding these sensations, including feeling ‘depressed at times, frustrated, concerned, embarrassed, young, glad and sexy’.
An additional 3/96 women had experienced three of the five PGAD criteria, but did not find the sensations intrusive or distressing. These sensations were associated with only positive emotions.
DISCUSSION
This study is the first to investigate how frequently sensations of spontaneous GA and PGAD are found in a female adult population. The finding of a single subject with all diagnostic criteria for PGAD in such a small sample suggests that PGAD is not exceptionally rare; however, larger studies would be required to confirm this statement as this study is not large enough to comment on population prevalence. It is plausible that with a longer period of data collection and with a larger study sample of respondents from the general population or from a different medical setting, different responses to these questions may have been noted.
This work however makes a number of interesting observations regarding GA, which furthers our understanding of this area of female sexual medicine. Firstly, a significant proportion of women experience spontaneous arousal of the genitals, in the absence of conscious desire or sexual excitement, which is not accompanied by any other features of PGAD. This phenomenon has not previously been well described and appears to challenge our understanding of the conventional sexual response cycle, where desire/excitement is a core phase. 11 Occurring at this high frequency in young healthy women, it is likely to represent part of the normative genital response, in a similar way to the male response.
Secondly, a small proportion of women were identified who reported multiple features of spontaneous and persistent GA, with chronicity over years, but who did not find the sensations distressing and indeed were associated with only positive emotions in some cases.
Owing to the small numbers of women with multiple features of persistent GA and PGAD, further conclusions cannot be drawn from this work. Additional shortcomings of this paper are the relatively high (but not atypical) refusal rate and the study population of young women attending this clinic. This sample may miss clusters of PGAD cases occurring within older age groups and in the peri/postmenopausal state. Furthermore, an awareness of the possibility of STIs in sexual health clinic attendees may increase anxiety and vigilance about other aspects of sexual or genital abnormalities and may have inflated the number of women reporting awareness of ‘spontaneous arousal’. However, the rates of anxiety in STI clinics are not higher than in medical outpatient departments or general practice. 12
Further research is clearly needed to establish the frequency of both spontaneous GA in women and PGAD in larger settings. Nevertheless, the results of this first study suggest that PGAD is not as rare as had previously been suspected. 13 As awareness of PGAD continues to grow, clinicians should remain vigilant to the possibility of medical and particularly psychological contributing factors. Clinical guidelines 14 will aid appropriate investigation and management.