
Abstract
Sexual health services in primary care, known in the UK as local enhanced services in sexual health (LESSH), aim to increase access to sexually transmitted infection (STI) screening and treatment. Little is known about the characteristics, quality or public health impact of these services. We identified national standards for service provision, and evaluated LESSH against them using a structure, process and outcome approach. Clinical structure and process standards were generally well met, with the exception of partner notification provision. However, public health and outcome measures were largely unascertainable and often undefined in the standards. If the primary care STI services are to deliver public health benefit, improved outcome measures and data collection are required.
INTRODUCTION
In the UK, sexually transmitted infection (STI) services have traditionally been provided in specialist genitourinary (GU) medicine clinics. Access to such clinics has been problematic as demand has increased, although recent efforts to achieve access within 48 hours have improved this. 1 The contribution of primary care to STI management has become apparent recently, but provision is highly variable. 2–4 The National Strategy for Sexual Health 5 set a policy direction towards improving STI services in primary care to increase capacity and patient choice, including provision of basic (‘level one’) services in most self-referral settings.
Local enhanced services in sexual health (LESSH) are a means of encouraging interested general practitioners (GPs) and other service providers to expand provision. The service specification and tariff are determined locally. The Department of Health has published an example specification. 6
A national postal survey of primary care trusts (PCTs) in England in 2007 found that 27% of the 80% of PCTs who responded, and 5% of their GP practices, offered LESSH, highlighting variation in uptake. 7 Within the LESSH, it is not known what services are offered, or to whom, or how they link to GU medicine services. It is important to understand the virtues and deficits of existing LESSH, in order to inform and rationalize the development of STI services delivered to populations.
The aims of this study are
To identify and describe the capacity and characteristics of STI services in Surrey and Sussex, particularly LESSH; To evaluate these services against identified national standards; To identify gaps in available standards; To inform future evidence-based development of LESSH.
METHODS
Summary of overall approach
Published standards for sexual health services were identified. The STI services in the population studied were located and described. Service delivery was evaluated against the identified standards.
Setting of study
Surrey and Sussex are neighbouring counties in the South East of England, with a combined population of 2.5 million. There are both rural and urban areas with affluent and deprived populations.
Identification of standards
Relevant documents were identified by discussion with experts and service leaders and from professional organizations. Inclusion required publication since 2001 by a national body. Standards that related to accessibility, capacity, clinical standards, staff training and competencies, monitoring and surveillance and costs were reviewed.
Identification of LESSH
GU medicine clinics were identified from the British Association of Sexual Health and HIV directory (
A questionnaire was developed to identify LESSH and assess capacity of GU medicine clinics, drawing on previous work on access to GU medicine services. 8,9 The questionnaire was piloted with consultants from another region and adapted before sending to GU medicine leads in eligible clinics by post. Commissioners were identified from the questionnaires or, where not known to GU medicine leads, by contacting PCTs. Semistructured interviews with commissioners were conducted in person or by telephone to identify further LESSH and obtain service specifications. Other service providers and managers identified by commissioners as involved with LESSH were also contacted and interviewed.
Evaluation of LESSH against published standards
Service specifications of LESSH were used as the basis for evaluation. Populations were defined by PCT except in the case of two neighbouring PCTs with a joint strategy on sexual health which were considered together. Using the established approach of Donabedian, standards were divided into structure, process and outcome. 10
Data processing and analysis
Data from the questionnaire were entered into a MS Access database and descriptive statistics derived using MS Excel. Interviews were recorded by hand.
Service locations and types were represented geographically using MapInfo Professional 8.0 (Pitney Bowes Software Inc., Troy, NY, USA), overlaid on PCT boundaries and Index of Multiple Deprivation (IMD) by local authority. The Local authorities were ranked by their national IMD rank and divided into quintiles.
GU medicine clinic and LESSH capacity in each PCT were derived from questionnaires, specifications and interview responses. The 16–44-year-old population in the PCTs was derived from single age year estimates for mid-2006, obtained from the Office for National Statistics by the Health Protection Agency. Capacity in GU medicine per 1000 residents aged 16–44 years was calculated. Routinely collected data (hospital outpatient activity) were sought to validate these estimates.
Ethical review
Ethical review was not required as the study was a planned service evaluation and did not require access to personally identifiable information.
RESULTS
Identification of standards
Twenty-two documents from six organizations met inclusion criteria. Forty-one standards were identified, 13 relating to structure, 17 to process and 11 to outcomes (Table 1).
Sources of standards identified
Multiple documents provide clinical guidelines and outline necessary training and competencies for staff involved in LESSH. Standards addressing provision for populations (capacity, accessibility) are more difficult to interpret for this setting. Accessibility guidelines focus mainly on GU medicine and 48 hour access (Table 2).
Identified standards and evaluation findings
Key: A = achieved; N = not achieved; U = unascertainable; NA = not applicable; GU = genitourinary; STI = sexually transmitted infection; LESSH = local enhanced services in sexual health; PCT = primary care trust
*See Table 1 for sources of standards
Notes:
1 Only two practices offering LESSH, representing only 1% GP practices in the PCT
2 GU medicine only, no LESSH in this PCT
3 Limited level 2 service access
4 One LESSH achieved for young people only, other does not
5 GU medicine achieved, not achieved for LESSH
6 An informal support arrangement is in place with one GP providing a LESSH and GU medicine
7 Full range of hepatitis screening and vaccination available only in GU medicine, limited in LESSH
8 Free STI treatment not specified for all LESSH
9 One LESSH reporting via GU medicine to KC60/GU medicineCAD. Others not reporting
According to guidelines, basic STI services should be available in the majority of self-referral settings, 5 but no standard for LESSH or STI testing capacity within primary care exists. Sexual Health Needs Assessment 11 is recommended to guide service provision. 12 All PCTs studied were undertaking such assessments and, until these are complete, it is difficult to define a standard for capacity or to measure its fulfilment. Standards identified for monitoring and surveillance are general rather than specific. The LESSH specifications reflect this, including little detail on data collection and reporting.
Results of surveys and interviews
The area studied includes five PCTs with 11 GU medicine clinics and seven GU medicine satellite services, mainly located in urban centres. Figure 1 shows the locations of services, in relation to PCT, local authority (shaded by IMD quintile) and urbanized areas.
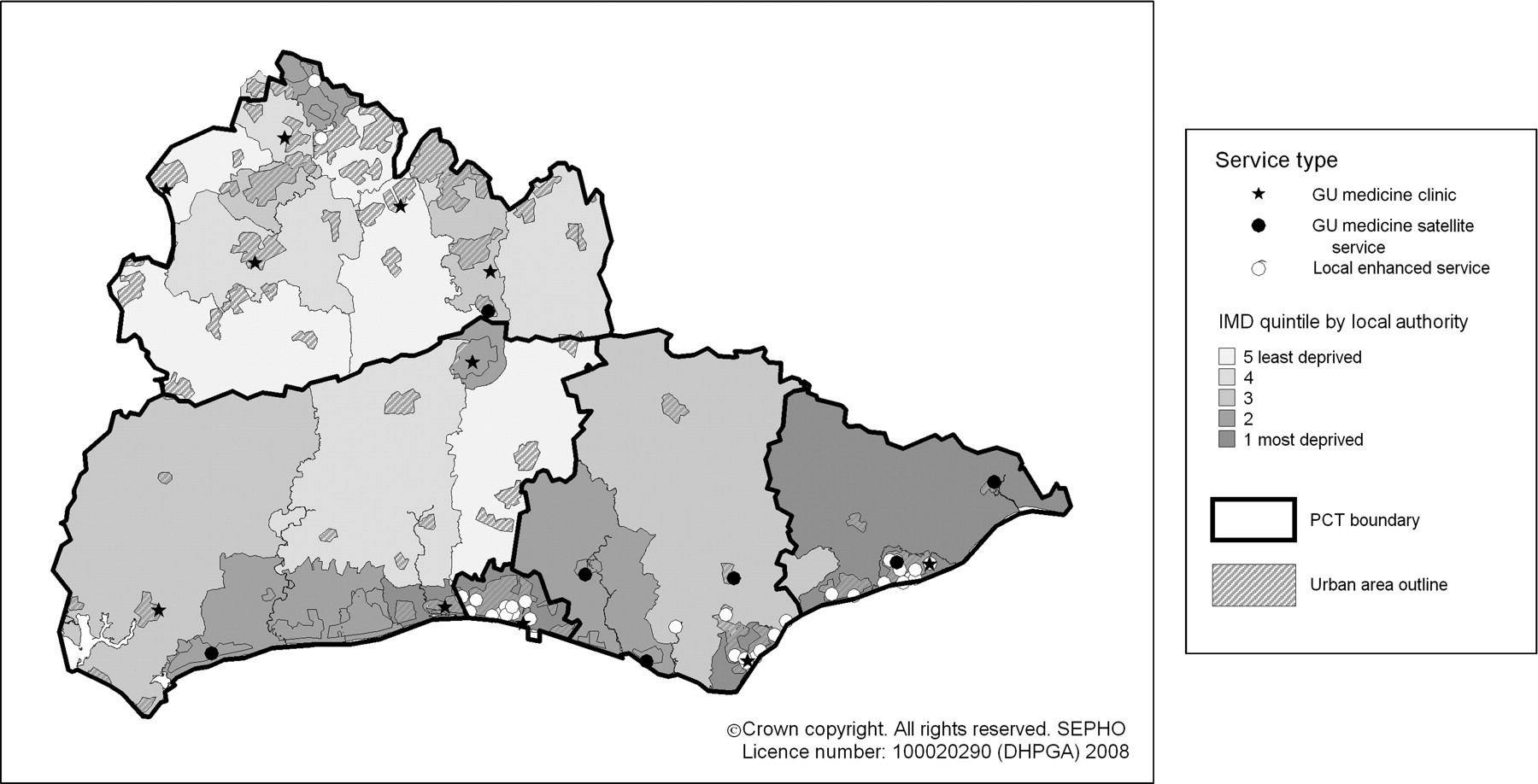
Location of sexual health services by primary care trust
All GU medicine consultants (11/11) in five PCTs responded to the questionnaire. All commissioners (4/4 as 2 PCTs share one commissioner) and 4/5 identified key personnel were interviewed. All PCTs emphasized that service configurations were likely to change in the near future.
Four out of five PCTs offered at least one LESSH but only two GU medicine consultants (11%) were aware of these, with only one able to give full details. All LESSH identified were located in GP practices (Figure 1).
There was wide variation in LESSH coverage, LESSH capacity and GU medicine capacity between PCTs (Table 3). No comparative data from routine National Health Service (NHS) outpatient activity statistics were available for GU medicine.
Comparison of LESSH coverage, LESSH capacity, GU medicine capacity and total capacity across PCTs in Surrey and Sussex
GU = genitourinary; LESSH = local enhanced services in sexual health; PCT = primary care trust
Notes:
1 Number of practices obtained from Health Commission website and verified using QOF data
2 16- to 44-year-old populations estimated from data obtained by Health Protection Agency from Office of National Statistics, based on mid-2006 population estimates
3 Based on information from genitourinary medicine consultant leads responding to questionnaire
4 LESSH specifications do not specify a target number of patients seen so no estimate could be made
5 Estimated by assuming both services have same capacity
Description of service specifications
Six different service specifications for LESSH were identified, four of which targeted young people (Table 4). Two specifications excluded partner notification, including only statements that links will be made in the future with GU medicine for this activity. However, the local GU medicine consultants were not aware of these services. Only one specification included specific staffing provision for partner notification.
Summary of LESSH specifications
GU = genitourinary; LESSH = local enhanced services in sexual health; PCT = primary care trust; UTI = urinary tract infection; GP = general practitioner
Evaluation of services (Table 2)
Standards relating to accessibility of services were largely met, as were those for staff training and competencies. Standards poorly met included those relating to service networks such as GU medicine support, shared protocols and clear referral pathways. Clinical outcome standards, e.g. treatment of diagnosed infections, were unascertainable, as data collection was poor.
DISCUSSION
Information is lacking on capacity and provision of LESSH in some areas, causing difficulties identifying services. This may be linked to the lack of specific standards for capacity.
There is variation in degree of coverage of LESSH, and in their scope and aims. This may make it difficult to monitor and evaluate the impact of these services on a regional and national level.
Data collection related to clinical outcomes within services is poor, preventing evaluation. Monitoring and surveillance requirements and systems are poorly specified, which may relate to the lack of detailed standards for STI monitoring in primary care.
Despite standards requiring involvement of GU medicine clinicians and defined care pathways for patients across networks, there is often poor co-ordination and a lack of formal links between LESSH and the local GU medicine clinics. This may be detrimental to patient care.
The majority of LESSH identified target young people, with LESSH provision for older adults and other risk groups, such as men who have sex with men, relatively lacking.
This structured evaluation against existing national standards provides a model for evaluation of community sexual health services. The varied geography and population in the area chosen allows a balanced view of LESSH implementation and findings should be generalizable to other parts of the UK. The excellent response rate validates the results.
The use of service specifications as the basis of the evaluation may not reflect the reality of service provision. Evaluation is also limited by the shortcomings of available standards. The 48-hour access standard may not deliver access for populations with travelling difficulties and close only to an occasional, but local, service. As many PCTs cover a wide geographical area, which is not necessarily well connected, it may be meaningless to have a service available somewhere in the PCT daily (standard 5) if some localities are served infrequently or never. Population data, geography and service characteristics need to be synthesized in standards for accessibility of STI services.
These data represent only a snapshot of the region studied as services change rapidly, for example, since conducting the study one LESSH specification has been withdrawn.
We were unable to obtain reliable data for GU medicine activity from the NHS outpatient activity monitoring data-set for comparison with the findings of the questionnaire. This is a compulsory data return and it is concerning that a large volume specialty such as GU medicine appears to be largely missing from it.
This is the first study to compare and evaluate STI provision, including LESSH, across several PCTs. Previous work identified the need for LESSH and support for implementation from GPs in East Berkshire, a relatively affluent area of the UK underprovided with GU medicine services. 13 A study in London assessed the impact of implementation of a LESSH on STI testing in general practice and found that although testing increased in participating practices, the difference in level of provision between these practices and non-participants also increased. 14 If a similar effect was seen in Surrey and Sussex, it could mean 99% of practices offering little STI care.
The problems of monitoring STI screening and treatment in primary care are well described. 15,16 Statutory reporting is not required and laboratory reporting (of positive diagnoses) is patchy and subject to bias. As primary care-based activity in sexual health increases, monitoring and surveillance become even more important to inform the national epidemiological picture.
LESSH are being used to drive provision of the basic STI services, which should be available in most primary care settings. 12 This may lead to basic services becoming optional extras, perversely worsening inequalities in access.
There is a general lack of data collection for audit/cost-effectiveness evaluation despite investment in LESSH. This makes evaluation of clinical outcomes, and effects on STI control difficult, threatening future STI control. Systems and support for monitoring and evaluation need to be built in to commissioning. Current implementation of a disaggregate reporting system in GU medicine clinics will greatly improve sexual health data. 17 Primary care-based services must not be left behind.
There is a need for a more joined-up approach to commissioning sexual health services in many areas. The identified lack of co-ordination may require urgent attention to care pathways.
Future work should include investigation of patient pathways through LESSH. If symptomatic individuals delay until their local service is open this may negatively affect STI control.
A comparison of the effect of different types and coverage levels of LESSH provision on STI control and GU medicine activity would provide useful evidence for planning future services.
Footnotes
ACKNOWLEDGEMENTS
We would like to thank those participating in the study, BASHH and the HPA for the honorary fellowship, which made this work possible and Briony Tatem at the South East Public Health Observatory for her help with maps.