
Abstract
Population-based surveillance data can help guide research priorities and plan programmes to prevent death among women with AIDS. We describe the predictors of mortality among women diagnosed with AIDS in Illinois, USA. Using the HIV/AIDS Reporting System), we identified 1944 adult women who were diagnosed with AIDS during January 1999–December 2004. The proportion of women who died within one year of diagnosis of AIDS declined from 97% in 1999 to 12% in 2005. Multivariate analysis indicated that age ≥45 years, intravenous drug use, diagnosis of clinical AIDS and hospitalization at the time of AIDS diagnosis were significant predictors of death among women with AIDS. The number of women who died soon after diagnosis with AIDS declined substantially. Nevertheless, prevention programmes designed to improve survival among women with AIDS should emphasize early diagnosis and referral for care in an effort to prevent first diagnosis with clinical AIDS during hospitalization.
INTRODUCTION
With the advent of highly active antiretroviral therapy (HAART) in 1996, progression from the diagnosis of AIDS to death has slowed considerably, and AIDS-associated hospitalization rates 1,2 and overall mortality rates have declined. 3–10 However, this decline has been delayed in women with AIDS and is smaller in magnitude than what is seen among men. 11
Historically, a number of factors have been shown to influence survival among persons with AIDS, including viral load, 12 age, 13 race, CD4 count, 4 prior hospitalization, 14 serum albumin, percent deviation from ideal body weight, number of co-morbidities at time of admission 15 and intravenous drug use. 16 Several of these factors may represent markers for differences in access to treatment, compliance or disease severity at diagnosis. 16 Furthermore, reported AIDS cases often include persons whose initial HIV diagnosis coincides with their AIDS diagnosis (so that they receive no or late access to HIV related, potentially life-prolonging medical care) and/or those who have failed treatment. 3
Few population-based surveillance data have been published examining mortality among women with AIDS. We describe the changing epidemiology of HIV/AIDS in Illinois (the US state with the 6th highest number of annual AIDS cases reported) during the HAART era. Data from the Illinois HIV/AIDS Reporting System (HARS) were analysed to describe the predictors of mortality among a cohort of women diagnosed with AIDS in Illinois. We focused our analyses on the time period following the broad availability of HAART. By examining the predictors of mortality among women with AIDS, we search for insight that will help to guide research priorities and planning programs to prevent death among women with AIDS.
METHODS
Study population
HIV/AIDS surveillance data are maintained through HARS, a collaborative effort between state and local health departments and the Centers for Disease Control and Prevention (CDC). In Illinois, health-care providers and laboratories report cases of HIV/AIDS to the local health department (using a standardized case report form) who then report cases to the state health department. 16 AIDS surveillance data are submitted monthly from the state health department to CDC. 12 HARS variables include mode of exposure to HIV, sex, race/ethnicity, age group, vital status, case definition category, hospitalization at time of AIDS diagnosis, referral for HIV-related medical services at any point in time and other information.
Using HARS, we identified 1944 women ≥18 years of age who were diagnosed with AIDS during 1 January 1999 to 31 December 2004 in Illinois. All women met the 1993 CDC AIDS case definition of immunological AIDS, a CD4 count <200 cells/μL or CD4 percent <14 or clinical AIDS. 17 For the purpose of our study, immunological AIDS was defined as a CD4 count <200 cells/μL or a CD4 percent <14 during 0–3 months following diagnosis with AIDS. Clinical AIDS was defined as any definitive or presumptive diagnosis with an AIDS indicator disease. 4 Our data-set included deaths reported to the Illinois Department of Public Health (IDPH) through 31 December 2005. Vital statistics matching for death data was performed each month for the duration of the study period. Nearly all CD4 counts were reported to IDPH by paper case report form, with the exception of one laboratory that began reporting electronically during 2003.
Statistical analyses
We used bivariate, stratified and multivariate analyses to identify the strongest predictors of all-cause mortality among women with AIDS. Logistic regression analysis included variables found to be significant in the bivariate analysis. SAS 9.1 for Windows (SAS Institute Inc., Cary, NC, USA) and Epi Info Version 3.3.2 were used for all statistical analyses. We prioritized analysis of risk factors associated with death, relatively soon after the initial diagnosis of AIDS, such as within only one month or one year, because prevention of these early deaths may substantially help increase the survival rate among women with AIDS.
RESULTS
At the time of AIDS diagnosis, the median age of the 1944 cases was 38 years (range, 18–86 years); 72% (1407/1944) were black, 15% (289/1944) were white, 11% (218/1944) were Hispanic and 2% (30/1944) were of other race. During the study period, 20% (382/1944) of the cases died with AIDS. The number of annual deaths among this cohort of women with AIDS steadily increased during 1999–2002 and peaked at 86 deaths in 2002, but decreased to 26 deaths in 2005. Of the women who died during the study period, 73% (280/382) were black, 15% (59/382) were white and 9% (34/382) were Hispanic. Among women who died, the proportion of women who died within one year of diagnosis of AIDS declined from 97% (35/36) in 1999 to 12% (3/26) in 2005 (Figure 1). The median number of years between diagnosis of AIDS and death was one year during 1999–2005. During 2004–2005, the median time period was two years.

Proportion of deaths among women within one year and one month of diagnosis of AIDS by year, Illinois, 1999–2005
The number of women with clinical AIDS alone decreased from 48 cases to 22 cases (46%) as did the number of women with both clinical and immunological AIDS (from 119 cases to 60 cases; 50%), whereas the number of women diagnosed with only immunological AIDS increased from 130 cases to 203 cases (56%) (Figure 2). The median CD4 count (during 0–3 months following AIDS diagnosis) for women diagnosed with immunological AIDS was 92 cells/μL (interquartile range [IQR], 27–161 cells/μL) and for women diagnosed with clinical AIDS, the median CD4 count was 48 cells/μL (IQR, 17–135 cells/μL). Sixty-six percent (161/245) of women hospitalized sometime after diagnosis with AIDS and who died with AIDS experienced an AIDS-defining condition. The most frequent AIDS-defining conditions diagnosed among women who were hospitalized and subsequently died with AIDS included Pneumocystis jirovecii pneumonia (23%; 56/245), recurrent pneumonia (18%; 43/245) and wasting syndrome (16%; 39/245).
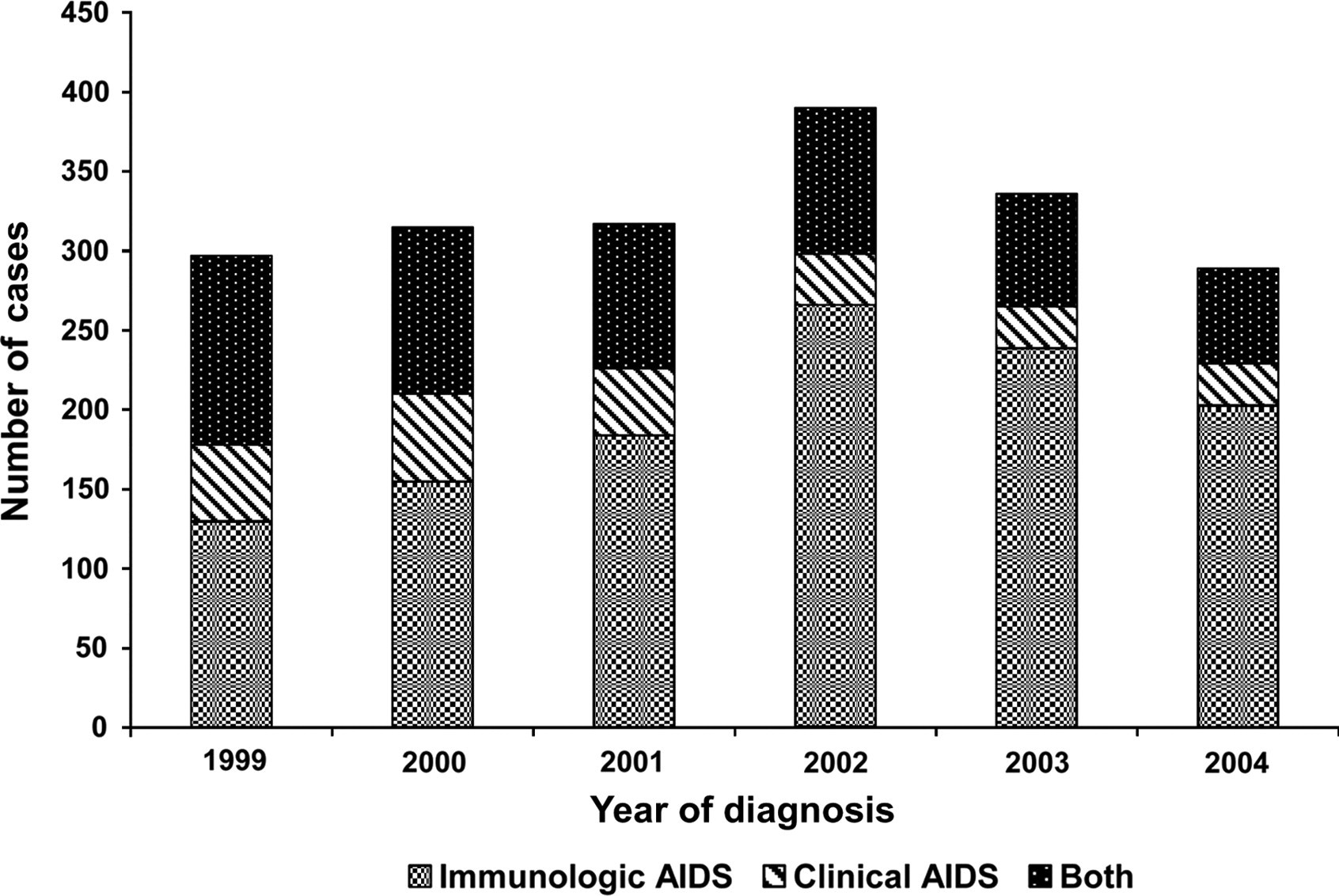
Number of women with immunological and/or clinical AIDS by year of diagnosis, Illinois, 1999–2004
By proportion, intravenous drug use (45%) was the most frequently reported mode of exposure among women who died during the study period, followed by heterosexual contact (35%). Women who were alive at the end of the study period reported heterosexual contact (51%) as the most frequent mode of exposure, followed by intravenous drug use (30%) (Table 1). Specifically, heterosexual contact with an HIV/AIDS-positive person was most frequently reported among women who reported heterosexual contact as their mode of exposure.
Frequency of HIV mode of exposure among women with AIDS in Illinois, 1999–2004
Bivariate analysis indicated that age ≥45 years (relative risk [RR], 1.7, 95% confidence interval [CI], 1.45–2.08), intravenous drug use (RR, 2.0, 95% CI, 1.56–2.52), diagnosis of clinical AIDS (relative risk [RR], 2.6, 95% CI, 2.15–3.19) and hospitalization at the time of AIDS diagnosis (RR, 2.7, 95% CI, 2.24–3.30) were all predictive of death among women with AIDS. However, African-American race was not associated with death (RR, 0.98, 95% CI, 0.76–1.26). Women referred for medical services (RR, 0.41, 95% CI, 0.29–0.59) or who reported having been diagnosed with HIV before their AIDS diagnosis (RR, 0.75, 95% CI, 0.63–0.90) were less likely to die with AIDS (Table 2).
Risk factors for death after AIDS diagnosis, Illinois, 1999–2004
*Number of cases in each category for which status (alive versus dead) was available
†Patients were diagnosed with clinical AIDS and immunological AIDS or only clinical AIDS
CI = confidence interval
We fit a logistic regression model including predictors found to be significant in the bivariate analysis. After adjustment, age ≥45 years (OR, 1.6, 95% CI, 1.11–2.19), intravenous drug use (OR, 2.1, 95% CI, 1.48–2.85), diagnosis of clinical AIDS (OR, 2.0, 95% CI, 1.47–2.83) and hospitalization at the time of AIDS diagnosis (OR, 2.7, 95% CI, 1.96–3.81) remained significant predictors of death among women with AIDS.
Bivariate analysis of women who died (n = 382) indicated that age ≥45 years of age (RR, 1.4, 95% CI, 1.22–1.69) and hospitalization at the time of AIDS diagnosis (1.6, 95% CI, 1.26–1.96) were significant predictors of death within one year of AIDS diagnosis. Receipt of antiretroviral treatment (RR, 0.72, 95% CI, 0.58–0.89), referral for medical services (RR, 0.52, 95% CI, 0.45–0.61) and diagnosis of HIV before diagnosis of AIDS (RR, 0.83, 95% CI, 0.70–0.98) were protective against death within one year of AIDS diagnosis (Table 3). Women ≥45 years of age were not significantly more likely (RR, 1.09, 95% CI, 0.92–1.30) than women 18–44 years of age to have had a CD4 count <50 cells/μL. Among women who died during January 1999–December 2005, 28% (106/382) died within one month of diagnosis of AIDS and white women were 1.6 times (95% CI, 1.10–2.33) more likely to die within one month of diagnosis of AIDS compared with black women (Table 3). However, the white women who died were generally older (46%; 27/59 were ≥45 years) than the black women who died (36%; 102/280 were ≥45 years), and only 34% (20/59) of the white women who died lived in Chicago compared with 77% (215/280) of the black women who died. Of the women who died within one month of diagnosis of AIDS, 68% (45/66) had received antiretroviral therapy. However, 38% (40/106) of responses were missing for this variable. The overall median CD4 count for women who died within one month of diagnosis was 35 cells/μL (range, 7 cells/μL in 2001–59 cells/μL in 2004).
Risk factors for death within one year and one month of AIDS diagnosis, Illinois, 1999–2004
*Number of cases in each category for which date of death and date of AIDS diagnosis were complete
†Patients were diagnosed with clinical AIDS and immunological AIDS or only clinical AIDS
CI = confidence interval
DISCUSSION
These AIDS surveillance data demonstrate a decline in the proportion of deaths among women within one year following the diagnosis of AIDS during 1999–2005. Among our findings, the data demonstrate that women who were hospitalized at the time of their AIDS diagnosis were more likely to die with AIDS compared with women who were not hospitalized at diagnosis. This may have been because women who were hospitalized were more severely ill (e.g. with an opportunistic infection). Our data underscore the importance of a risk factor assessment which demonstrated that women with a history of intravenous drug use had a greater risk of death. 16 This finding may be related to high-risk lifestyle factors, co-morbidity (such as hepatitis B or C virus infection) or overdose. Active intravenous drug use has been found to be associated with underutilization of HAART. 18 Several factors likely contribute to underutilization, including the effects of drug addiction on lifestyle stability, lack of social support, mistrust of the medical system and clinician discomfort in treating intravenous drug users. 18 Women ≥45 years of age with AIDS were more likely to die compared with women of 18–44 years of age. Factors contributing to the growing incidence of HIV/AIDS in the older age bracket include decreased knowledge of transmission and risk, ongoing high-risk behaviour, changes in mucosal barriers and immune function, which facilitate transmission, and suboptimal preventive and screening efforts. 19 Older persons also may have had HIV/AIDS for a longer period of time prior to initial diagnosis. Our data did not find black race to be a significant predictor of death among women with AIDS, possibly because the study time period was a number of years into the treatment era and Illinois has a relatively generous AIDS Drug Assistance Program that may be helping to offset the racial disparity observed previously. 20 It is also possible that white women with AIDS in Illinois have similar characteristics, relevant to risk for death, that black women may have (e.g. injecting drug user, advanced clinical presentation, lack of substantial income and insurance).
Comparative analysis of only women who died revealed that women who died within one year and women who died within one month of AIDS diagnosis displayed a risk factor profile similar to that of the entire cohort of women (e.g. age ≥ 45 years, hospitalization at time of AIDS diagnosis). One exception was that women who received antiretroviral treatment had a decreased risk of death within one year of AIDS diagnosis (also true for death within one month of AIDS diagnosis), which was not found to be true when examining predictors of death among the entire cohort regardless of time since the diagnosis of AIDS. Another finding was that white women were more likely to die within one month of AIDS diagnosis compared with black women. This may be explained in part by the fact that the white women who died were older than the black women who died, and only 34% of the white women who died lived in Chicago compared with 77% of black women who died. HIV health-care specialists and facilities devoted to HIV-related care are more accessible and abundant in Chicago than in other areas of the state. Women who died with AIDS within one month of diagnosis generally had substantially low CD4 counts.
A limitation of our study is that the cause of death was not included; therefore, we do not know how many women died of non-AIDS-related issues. Cause of death information has become increasingly more important when examining predictors of mortality among persons with AIDS given that a significant contribution of mortality is from non-AIDS-defining illnesses. 13,21,22 Also, because reports of deaths among persons with HIV/AIDS are sent to IDPH some time after a death has occured, we may have missed deaths that occurred among this cohort of women during the study period but were not reported until after 31 December 2005.
Antiretroviral therapy has delayed progression to death among women with AIDS. However, prevention or outreach programmes designed to improve survival among women with AIDS should emphasize early diagnosis and referral for care so that women are not first diagnosed as clinical AIDS and hospitalized. Pneumocystis pneumonia as the predominant AIDS-defining condition among this cohort of women further highlights the importance of identifying HIV infection early and initiating care. 23 Pneumocystis pneumonia is preventable with effective usually inexpensive and widely available antimicrobials. Physicians and other health-care providers play an important role in prevention. Systematic risk assessments should be part of routine care for these patients, including those for high-risk sexual activity and intravenous drug use and testing of older women, especially those with risk factors, to find infected women earlier. Testing pregnant women and women diagnosed with a sexually transmitted disease (STD) or tuberculosis may also result in earlier diagnosis. Other important prevention activities include referring patients for services such as substance abuse treatment, facilitating partner notification, providing education on HIV transmission, treating other STDs and prescribing prophylaxis for opportunistic infections such as P. jirovecii pneumonia.
Future research should be focused on determining the specific causes of death among women dying with AIDS including the possibility of drug overdose. Surveillance data should continue to be examined periodically for trends and factors associated with death among women with AIDS.
Footnotes
ACKNOWLEDGEMENT
We thank Dr Mardge Cohen for her useful comments on this manuscript.
This study was supported in part by CDC/CSTE Cooperative Agreement U60/CCU007277.