
Abstract
A 24-year-old lady presented to an evening genitourinary (GU) clinic with a short history of vulval and anal irritation. On perianal examination, several threadworms were visible. Symptoms resolved with oral mebendazole and strict personal and environmental hygiene. Threadworm is a common and easily treatable cause of pruritis ani, yet is underreported in GU literature. If the history is suggestive, consider performing the diagnostic cellophane test and/or prescribing empirical treatment.
CASE
A 24-year-old Caucasian female attended our evening genitourinary (GU) medicine clinic with a two-day history of vulval and perianal itching, worse nocturnally. She had no other associated symptoms or significant past medical history, and had self-medicated using topical clotrimazole cream with minimal relief. During genital examination, several white threadworms were visible perianally. Examination was otherwise unremarkable and a full sexual health screen was negative. She received oral mebendazole and followed strict hygiene advice. Symptoms resolved within four days. Her only sexual partner was untraceable and she reported no contact with children or persons with threadworm.
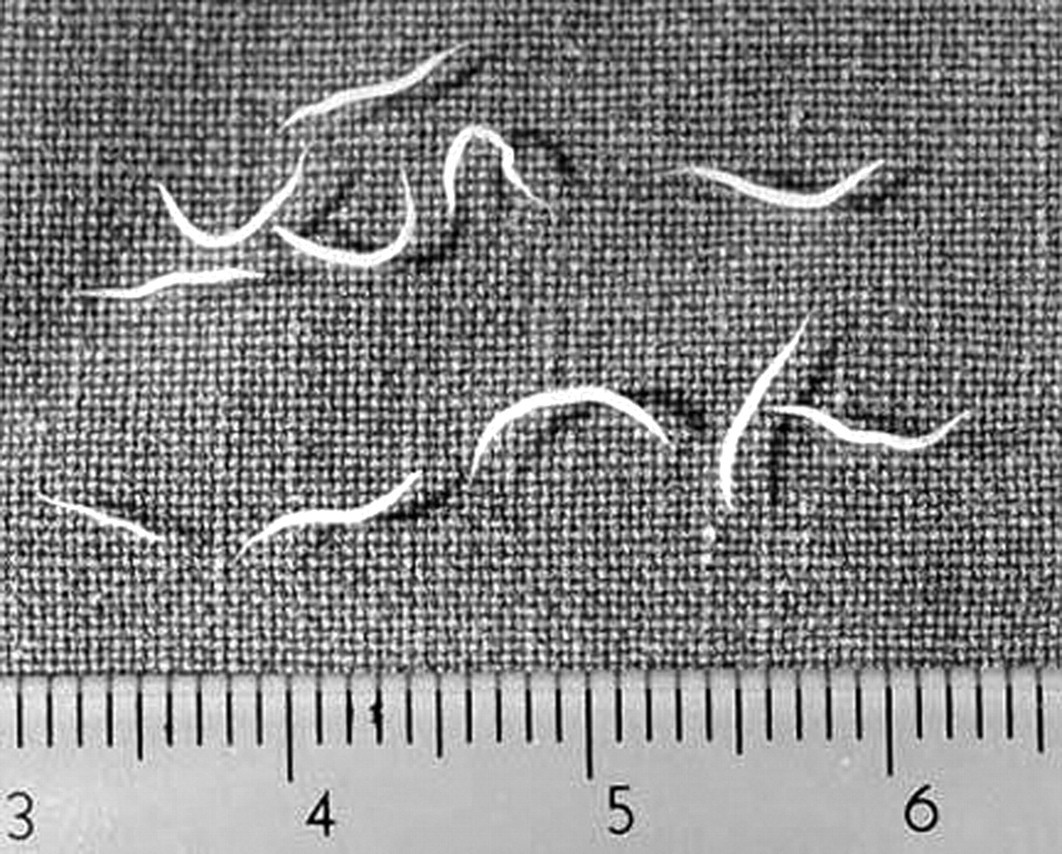
Threadworms. Adult males measure 2–5 mm and adult females measure 8–13 mm in length
DISCUSSION
Threadworm infection, also known as pinworm or enterobiasis, is caused by the organism Enterobius vermicularis (Figure 1). It accounts for over 200 million infections globally and is the commonest intestinal parasite in the UK. 1 Owing to inattention to good personal hygiene and close peer contact, the condition is more common in children than in adults. Persons living in overcrowded conditions, institutions or with an infected person are particularly affected. Transmission among families can be as high as 75%. 2
Threadworm is transmitted faeco-orally. These slender, white nematodes measure up to 13 mm long, reside and mate in the large bowel and can survive intestinally for six weeks. After mating, gravid females venture outside the anus and deposit their eggs perianally or occasionally in the vagina or female urethra. 1 Host inactivity such as resting or sleeping encourages this migratory process and thus worms are usually not visualized externally during the day.
Eggs stick to fingers or underneath the fingernails during scratching or wiping after defecation and are transferred to other persons by direct contact or via contaminated food, bathrooms, furniture or laundry. Infestation has been acquired from inhaling and then swallowing airborne eggs. Eggs can survive outside the human host for up to three weeks, during which time if swallowed they hatch in the small intestine.
Infected persons may experience itching around the anus (and/or vagina), which can be intense and more prominent at night; disturbed sleep/insomnia and irritability; anorexia and weight loss; and the passage of ‘white cotton threads’ in the bowel motions. Asymptomatic infestation is common and contributes to transmission.
Complications include secondary bacterial infection and vulvovaginitis. Severe morbidity is rare but can occur with ectopic or invasive infection. Ectopic sites with granuloma formation have been reported in the female genital tract, peritoneum, liver and lungs. 3–5 Invasive complications include pelvic inflammatory disease, appendicitis and eosinophilic colitis/gastroenteritis. 3,5–7
Differential diagnoses include anal fissure, contact or seborrhoeic dermatitis, atopic eczema, candida, tinea cruris, haemorrhoids and lichen planus. Threadworms are rarely confused with other worm infestations: human roundworms are approximately 30 cm long and tapeworm segments (proglottids) look like chains or single grains of rice.
Diagnosis is by direct visualization of worms in the perianal area or by performing the cellophane tape test (Graham test) (Figure 2). This involves firmly pressing a length of cellophane to the skin around the anus every morning and then placing on a slide for microscopy to identify ova. The test has a relatively low yield unless several tests are performed over consecutive days (sensitivity is 50% for one, 90% for three and 99% for five examinations) and so empirical treatment is often provided if the history sounds suggestive. 5 Eggs can occasionally be seen in samples taken from under the fingernails but are rarely found in urine or faecal specimens.
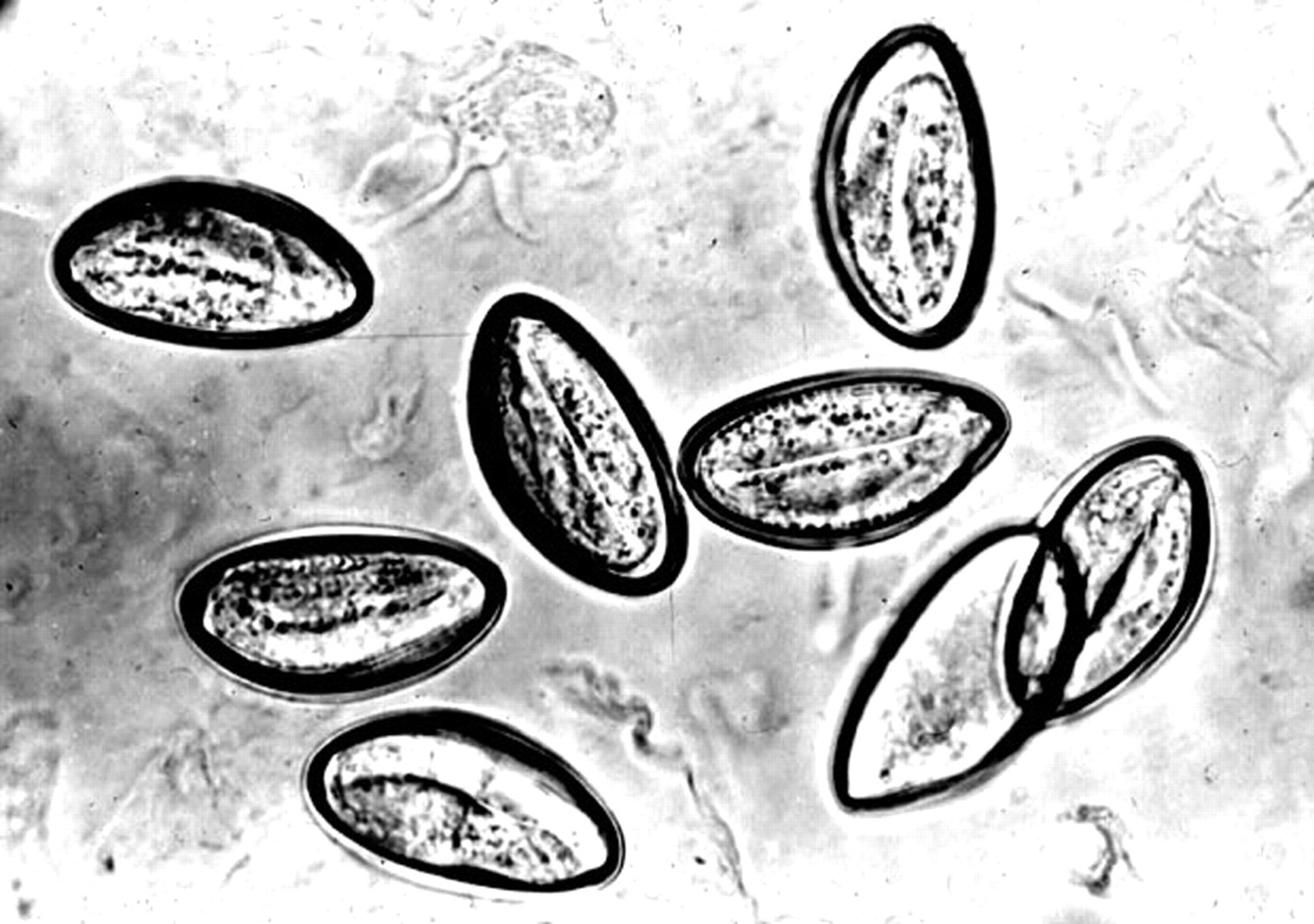
The cellophane test. The eggs usually measure 50–60 µm by 20–30 µm and contain larvae. They are not visible to the naked eye
The anti-helminth single dose oral treatments mebendazole or piperazine are thought to have comparable efficacy rates (90–100%) but are not effective against the eggs, specifically those swallowed or deposited externally; hence a second treatment is advised at two weeks. 1 Adjuvant strict personal and environmental hygiene is essential for at least two weeks (Table 1). For those declining or unable to take antihelminth therapy, strict hygiene alone may eradicate the infestation if continued for six weeks. All family members are advised to be treated even if they are asymptomatic. Unfortunately, re-infection is common.
Strict personal and environmental hygiene advice for the treatment of threadworm
Heterosexual transmission of threadworm has been reported and could be implicated in this case. 8,9 Threadworm is a common and easily treatable cause of ano-genital irritation, yet it hardly features in the GU medicine literature. The worm's nocturnal activity may partially explain its absence or underreporting during daytime GU services and its presence here during an evening clinic. One should have a high index of suspicion and consider the Graham test and/or empirical treatment in cases with a suggestive history.