
Abstract
Hepatitis A virus (HAV) and hepatitis B virus (HBV) continue to be major health concerns among men who have sex with men (MSM). The Internet both facilitates high-risk sexual encounters and provides opportunities for promoting healthy behaviours. This study compared self-reported HAV and HBV vaccination levels, based on demographics, health characteristics, hepatitis knowledge, attitudes and risk behaviours among MSM using an online survey posted from February through June 2005. Each participant (n = 968) reported whether they were vaccinated, infected or susceptible for hepatitis A and/or for hepatitis B. Men whose healthcare provider recommended vaccination were 12.91 (95% confidence interval [CI] 8.11, 20.55) times more likely to be vaccinated against HAV and 17.93 (95% CI 10.82, 29.70) times more likely to be vaccinated against HBV than those at risk of infection, respectively. These data provide essential information for public health professionals to successfully promote vaccination among members of this population.
Introduction
Hepatitis A is caused by a virus (HAV) that causes an acute infection that usually lasts a few weeks and may be subclinical. Hepatitis B is caused by a different virus (HBV) and can cause symptoms that range in severity from a mild illness, lasting a few weeks (acute), to a serious longterm (chronic) illness that can lead to liver disease or liver cancer. While rates of HAV and HBV infections have declined among many populations in the USA, the proportion of nationally reported acute cases that were attributed to high-risk populations, such as men having sex with men (MSM), have increased.1,2 The Centers for Disease Control and Prevention (CDC), the Gay and Lesbian Medical Association, and other public health experts and organizations recommend that MSM receive hepatitis A and B vaccinations.3–5 Across the USA, some professional requirements (e.g. healthcare workers) and some states (e.g. public schools) mandate vaccination. Despite these guidelines and mandates, as well as ample supply and availability of effective hepatitis A and B vaccines that prevent infection, vaccination coverage rates remain inadequate among MSM in the USA.6,7
Some studies have found that MSM who seek and find sexual partners on Internet websites may be at increased risk of acquiring sexually transmitted infections (STIs) compared with those who find partners elsewhere.8–11 MSM who responded to online surveys compared with men who completed surveys in community settings were more likely to report high-risk sexual activities and previous STIs, including HIV.12–14
However, we know little about the demographic and health characteristics, specifically about the hepatitis vaccination status, of the online MSM population. 15 In fact, little is known about hepatitis among the MSM population as a whole in the USA, because few population-based studies have asked, collected or reported data regarding sexual orientation. More information is needed to: a) describe the hepatitis-related characteristics of the online MSM population, and b) to serve as baseline data with which to compare future studies, and c) to inform future online or other interventions.
To address these issues, a study was conducted to measure demographics, and hepatitis vaccination-related health characteristics, knowledge, attitudes, risk behaviours and vaccination intentions by surveying a robust sample (defined as more than 200 participants) of MSM online.
Methods
Measures
Measures were developed by an iterative process of defining research questions, reviewing the literature, gathering expert review (n = 14), conducting cognitive interviews (n = 4) and pilot testing (n = 264). Survey questions were revised, shortened and clarified. The final survey consisted of between 40 and 69 questions: seven demographic, four health characteristic, 19 knowledge, four attitude, four risk behaviour and two questions about intentions to vaccinate. Total numbers of questions per survey varied depending on self-reported risk; if a participant was already immune to hepatitis A, for example, he was branched to the hepatitis B questions. The study methods and measures received unconditional approval by the Copernicus Group Independent Institutional Review Board.
Sample recruitment
The survey was posted on GayHealth's website for a period of four months from February to June 2005 and banner advertisements and promotions were placed on both www.GayHealth.com and www.ASHAstd.org. Data were collected on GayHealth.com's server and responses were maintained in an anonymous database. No compensation was offered for survey completion.
Analyses
Of the people who reviewed the online survey, 1237 consented to participate. Participants were restricted to male respondents aged 16 years or older, who lived in the USA. Of those who consented, 968 met the eligibility criteria. To see if knowledge, attitudes and behaviours were significantly different based on immune status, each respondent was categorized into one group regarding hepatitis A (vaccinated, infected or susceptible), and one group regarding hepatitis B (vaccinated, infected or susceptible). This study did not differentiate between acute and chronic infection when we asked participants if they had been infected with hepatitis B. A participant was classified as ‘vaccinated’ if he reported having had one or more vaccine doses. Those who reported prior infection were classified as ‘infected’. Men who said they were ‘not sure’ of their vaccination status were classified as ‘susceptible’. Descriptive analyses are shown for both the entire sample and those who reported infection with either hepatitis A or hepatitis B. Analyses were then restricted to a comparison of those who were susceptible and those who reported HAV and/or HBV vaccinations. Participants were dropped from the final analysis of HAV due to reported HAV infection (n = 56) and missing data from covariates of interest (n = 428). Participants were dropped from the final analysis of HBV due to reported HBV infection (n = 74) and missing covariates of interest (n = 418). In addition, the entire sample was restricted to those individuals who reported being susceptible to HAV or HBV infection and did not plan to be vaccinated, to determine perceptions about vaccines in this target group.
Bivariate analyses were conducted between immune status and other variables of interest, using χ2 tests. Unadjusted odds ratios were calculated between HAV or HBV susceptibility and variables significant in the bivariate analyses. As age group and education level were categorical variables, the age group of 45+ and reaching a high school education level were used as referent categories. Multivariate logistic regression was conducted to determine the association between a healthcare provider recommending HAV or HBV vaccination and vaccination status.
Analyses were conducted in SPSS® (version 11.0; SPSS Inc, Chicago, IL, USA) and Stata (version 9.2; StataCorp, College Station, TX, USA).
Results
Entire sample
The sample of MSM answering the questionnaire (n = 968) included 19.9% youth aged 16–24 years, 24.9% aged 25–34 years, 27.9% aged 35–44 years and 27.3% aged 45 years or older. The sample was well educated, as over half (56.7%) reported having attended at least some college. The majority of the sample (83.5%) was white, 7.1% identified as Latino or Hispanic and 57.3% lived in urban areas. Almost 30% reported HAV vaccination while over one-third reported HBV vaccination. About one-quarter (24.6%) reported vaccination for both HAV and HBV while 53.6% were not vaccinated for either virus.
Infected with HAV or HBV
Fifty-six individuals (5.8%) reported having been infected with HAV, and followed the general demographic patterns of the entire sample. The majority was aged 35 years or older (71.4%) and reported having at least 40 lifetime sexual partners (80.4%). Of those who were infected by HAV but not HBV and not vaccinated against HBV (n = 8), 75% did not plan to become vaccinated against HBV in the future.
Seventy-four individuals (8%) reported having been infected with HBV, and followed the general demographic patterns of the entire sample, except that only 1.85% (n = 1) were Latino. As with those men with HAV, the majority was aged 35 and older (75.7%) and reported at least 40 lifetime sexual partners (73.8%). Of those who were HBV infected but not infected with HAV nor HAV vaccinated (n = 32), 46.9% did not plan to become HAV vaccinated.
There were many similarities between the two infected groups. As expected, older men reported having greater numbers of sexual partners than younger men. Both groups were well connected to healthcare services and had extensive knowledge of health complications associated with HAV and HBV infection. Over 80% of each group reported having current health insurance, having a regular healthcare provider and having seen this provider in the past 12 months. About two-thirds (66.1% for HAV infected, 66.2% of HBV infected) of the individuals reported ever being diagnosed with an STD. At least 84% of both groups knew that HAV and/or HBV could cause liver damage and yellowing of skin. Past HAV infection was associated with HBV infection. Those reporting previous HAV infection were 11.34 (95% confidence interval [CI] 6.21, 20.69) times more likely to report HBV infection than those not reporting HAV infection (Figure 1).
Percentage of men having sex with men who self-reported hepatitis A and B vaccination status, of the entire sample, 2005. HAV = hepatitis A virus; HBV = hepatitis B virus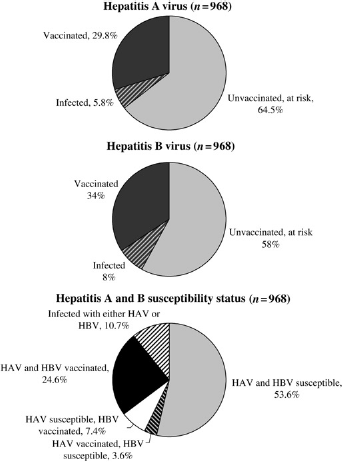
Comparison of individuals vaccinated or susceptible to HAV
Out of the entire dataset, 94.2% had not been previously infected with HAV and of those, 68.4% reported not being vaccinated and 31.6% reported being vaccinated against HAV. The following section will compare these two groups. Bivariate analyses found significant differences between vaccination status and having current health insurance, having a healthcare provider, having seen a provider in the past 12 months, ever being tested for or diagnosed with an STD, history of disclosing sexual behaviours to provider and recommendation by provider to become vaccinated (Table 1). Over 60% of all individuals at risk for HAV provided correct answers to knowledge about vaccine availability and modes of transmission for HAV or HBV. Those individuals who reported HAV vaccination also reported much higher levels of correct knowledge of vaccine availability and risk factors (Figure 2).
Demographic and healthcare characteristics of men who have sex with men vaccinated against and susceptible to hepatitis A virus infection
χ2 test P value <0.05
Missing <5% of data
Missing 12–16% of data
HCP = healthcare provider, STD = sexually transmitted disease
Correct knowledge of vaccine availability and routes of transmission for those susceptible to hepatitis A and hepatitis B infection. HAV= hepatitis A virus; HBV= hepatitis B virus
Unadjusted odds ratios indicated the association between demographics and being at risk for HAV infection. Self-reported HAV vaccinated individuals were 1.90 (95% CI 1.11, 3.25) and 2.09 (95% CI 1.43, 3.07) times more likely to have been tested for STDs or to have ever been diagnosed with an STD, respectively, than those individuals susceptible to HAV infection (Table 1). Individuals who disclosed their sexual activities to their healthcare provider were 2.36 (95% CI 1.56, 3.56) times more likely to be vaccinated against HAV than those susceptible to HAV. The influence of healthcare providers in encouraging vaccination is clear. Adjusting for age and education level, those individuals who reported that their healthcare provider recommended an HAV vaccination were 13.95 (95% CI 8.63, 22.55) times more likely to be vaccinated against HAV than their susceptible counterparts.
Comparison of individuals vaccinated or susceptible to HBV
Out of the entire dataset, 92.4% had not been infected with HBV and of those, 62.9% reported not being vaccinated and 37.1% reported being vaccinated against HBV. The following section will compare the vaccinated and susceptible groups. Bivariate analyses found significant differences between the distributions of vaccination status and age, number of lifetime partners, having current health insurance, having a regular healthcare provider, having seen a provider in the past 12 months, ever being tested for or diagnosed with an STD, history of disclosing sexual behaviours to provider and recommendation by provider to become vaccinated (Table 2). Individuals at risk for HBV infection also had lower levels of knowledge about vaccine availability and modes of transmission for HAV and HBV than their vaccinated counterparts (Figure 2).
Demographic and healthcare characteristics of men who have sex with men vaccinated against and susceptible to hepatitis B virus infection
χ2 test P value <0.05
Missing <5% of data
Missing 13–16% of data
HCP = healthcare provider, STD = sexually transmitted disease
Unadjusted odds ratios were calculated to determine factors associated with HBV vaccination or susceptibility. Those who reported vaccination were more likely to have visited a healthcare provider in the past year or to have been tested or diagnosed with STDs. Those who reported HBV vaccination were 2.20 (95% CI 1.31, 3.69) times more likely to have a regular healthcare provider than those who were susceptible (Table 2). As seen with those vaccinated against HAV, connection with a healthcare provider was associated with HBV vaccination. Those who reported HBV vaccination were 2.75 (95% CI 1.81, 4.16) and 17.93 (95% CI 10.82, 29.70) times more likely to have disclosed their sexual behaviours to their healthcare provider and been counselled to receive HBV vaccination, respectively, compared with those unvaccinated.
Vaccine perception
Beliefs surrounding vaccination are reported for those who did not report HAV or HBV vaccination and did not plan to become vaccinated. Among those at risk for HAV and HBV, high percentages reported a belief that vaccines are protective (79.6% for both) and self-efficacy to complete the vaccine regimen (64.7% and 64.0%, respectively). A little less than half of all men reported that they would feel safer with their partner if vaccinated against either virus (range: 43.7–45.6%). Low numbers of men at risk for HAV and HBV infection felt that vaccines were too costly (11.0% and 10.6%, respectively) (Figure 3). However, only 13.7% of HAV susceptible and 11.8% of HBV susceptible men reported plans to obtain vaccination.
Perceptions about vaccines among those not vaccinated for either HAV or HBV, respectively. HAV = hepatitis A virus; HBV = hepatitis B virus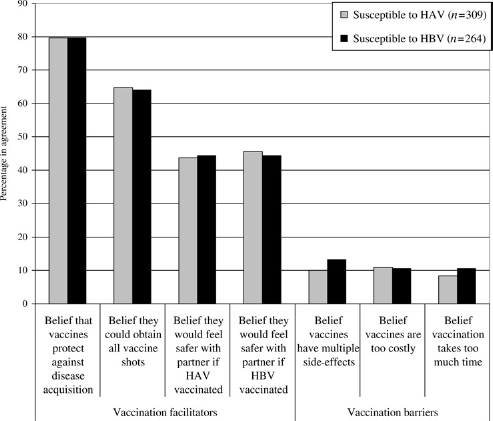
Discussion
Of this sample of online MSM, participants were predominately aged 25–44 years, well-educated, urban, and non-Hispanic Caucasians. The majority of the respondents reported high levels of income, having health insurance and a regular healthcare provider, and having visited a healthcare provider within the last 12 months. More than half of the respondents were susceptible to HAV and/or HBV infection (i.e. reported neither prior infection nor vaccination). Having a healthcare provider recommend vaccination was highly related to reported vaccination among this group of online MSM. Of those not vaccinated, there appeared to be few reported barriers to obtaining vaccination.
Recent CDC guidelines advocate for both HAV and HBV vaccination among MSM.3–5 Although the route of transmission differs between hepatitis viruses, 16 MSM are at risk for both diseases. Indeed, in this study, those who reported HAV infection were more than 11 times more likely to also report HBV infection; a finding mirrored in other studies. 6 The large association between dual infections among this sample strengthens the importance of tying prevention and vaccination messages for the two infections together. In addition, the use of the combination HAV/HBV vaccination would increase adherence to obtaining the full regimen of vaccination shots for full protection.6,17,18
In addition to response to a survey on one of two websites related to sexual health issues, this sample of men reported high levels of health insurance, having a healthcare provider, having seen that provider in the past year and having been tested for STDs. Taken together, these factors indicate a group highly connected to healthcare services and resources. Identification of a regular healthcare provider and recent healthcare visits may be an indication of some type of relationship with their provider. Indeed, 63.6% of HAV vaccinated men and 63.3% of HBV vaccinated individuals reported that they disclosed their sexual behaviours with their healthcare provider while only 27.4% of HAV susceptible and 40.7% of HBV susceptible men reported similar disclosure. In addition, healthcare provider recommendation for vaccination was strongly associated with reported vaccination status. Fostering this relationship between healthcare provider and patient provides opportunity for disclosure and potential adoption of preventive behaviours suggested in the course of discussions concerning sexual behaviour.
Several studies have linked health behaviour models to hepatitis vaccination acceptance18–22 and actual vaccination.15,22 This study, however, is one of the first to ask questions about vaccination intention along with attitudes to vaccination among the same sample of men. Low percentages of men who were susceptible to either HAV or HBV infection reported low levels of knowledge about the availability of hepatitis vaccination and transmission routes for either infection. However, high percentages of men reported belief in the efficacy of vaccines, belief in few side-effects from vaccines and the belief that vaccines are offered at an acceptable cost. Over 60% of men susceptible to either infection reported high self-efficacy or belief they could complete the vaccination regimen. These groups of susceptible men are a prime target for education and intervention campaigns. Those who disclosed their sexual behaviour to their healthcare provider, believed that vaccines are beneficial, and had not received vaccine recommendations are optimal candidates for an effective intervention, conducted by providers.
At the same time, interventions aimed at MSM should encourage men to seek supportive healthcare providers and to disclose appropriate information about sexual activities during healthcare visits to optimize proper care. The study findings indicate that interventions should emphasize modes of transmission differentiated by the two types of hepatitis, vaccine availability by hepatitis type, consequences of infection (e.g. liver damage), the need for vaccination among MSM and the number of MSM who have been vaccinated (making vaccination normative).
Collecting data from MSM online was quick, inexpensive and efficient; however, little is known about those who chose not to participate. Anonymous data collection through an online venue may help to decrease social desirability bias as respondents may feel more comfortable answering a computer survey than a face-to-face interview. However, this study is limited in the ability to generalize to all MSM populations, as it was a self-selected group of men who were visiting health websites and therefore may be more health conscious or have other characteristics that differ from the overall MSM population. Second, some of the demographic questions had large non-response rates. This may be because the questions appeared at the end of the study. Prior studies have shown that reported and actual vaccination status may differ, sometimes through exposure to an incomplete vaccination series. 6 The lack of serologic testing precludes the ability to validate immunity or prior infection status among this sample, and may have led to misclassification of vaccination status.
As expected, MSM who reported having health insurance, having a regular healthcare provider, having seen a provider in the last 12 months or having ever been tested for or diagnosed with an STD were more likely to have been vaccinated with hepatitis A or hepatitis B, or both. This confirms the importance of the healthcare visit and the recommendation of a provider. Future efforts need to focus on reaching healthcare providers and motivating them to discuss and recommend hepatitis vaccines, as appropriate. In addition, the fact that hepatitis vaccinations are available free of charge for those at risk, for example, at Pride events, through pharmaceutical companies, and at some public health clinics needs to be communicated to both MSM and their healthcare providers. Also, these data highlight the importance of increasing comfort levels of both providers and patients so that an environment conducive to disclosure of sexual activities can be fostered. Future research is needed to understand why a substantial percent of MSM who are susceptible to hepatitis do not intend to receive vaccinations, and how to overcome these objections.
Footnotes
Acknowledgement
This study was supported by Centers for Disease Control and Prevention (CDC) Cooperative Agreement No. U50/CCU423253-05.