
Abstract
We report the case of a patient with a large Buschke–Lowenstein tumour which had previously recurred following local excision. A preferred treatment modality for this rare variant of human papillomavirus has not been clearly defined. Treatment with chemo-radiotherapy in this case resulted in complete resolution of the disease without the need for further surgical intervention.
CASE REPORT
A 46-year-old man presented with a history of recurrent extensive perianal warts and surrounding abscess formation. In the previous 12 months, he had undergone examination under anaesthetic (EUA) on four occasions with excision of the perianal warts and incision and drainage of the abscesses. At the time of transfer, the lesion was causing considerable pain and there was significant bleeding from the affected area. Further EUA and biopsy revealed extensive disease with giant florid warts in the right ischio-rectal area extending downwards towards the scrotum (Figure 1).

Lesion before (a) and after (b) chemo-radiotherapy
Histopathology reported features of condyloma acuminatum with dysplasia amounting to anal intraepithelial neoplasia (AIN) 3 in areas, but there was no evidence of invasive malignancy. In situ hybridization for human papilloma virus (HPV) genotypes was requested and confirmed HPV 6 and HPV 11. A diagnosis of an HPV 6 and 11 positive condyloma acuminatum with AIN 3 was made and therefore confirmed a Buschke–Lowenstein tumour.
Magnetic resonance imaging showed a huge soft tissue mass measuring 8 × 12 × 13 cm arising from the left lower aspect of the anal canal, which extended across the midline, compressing but not invading the gluteal fat on the right side (Figure 2).The patient was also noted to have widespread fungal nail disease, suggesting some deficit in cell-mediated immunity. However, a T-cell count and differential showed CD3 1.100 × 109 (79%), CD4 0.874 × 10 (63%) and CD8 0.205 × 109 (15%), which are all within the normal range. An HIV antibody test was also negative.
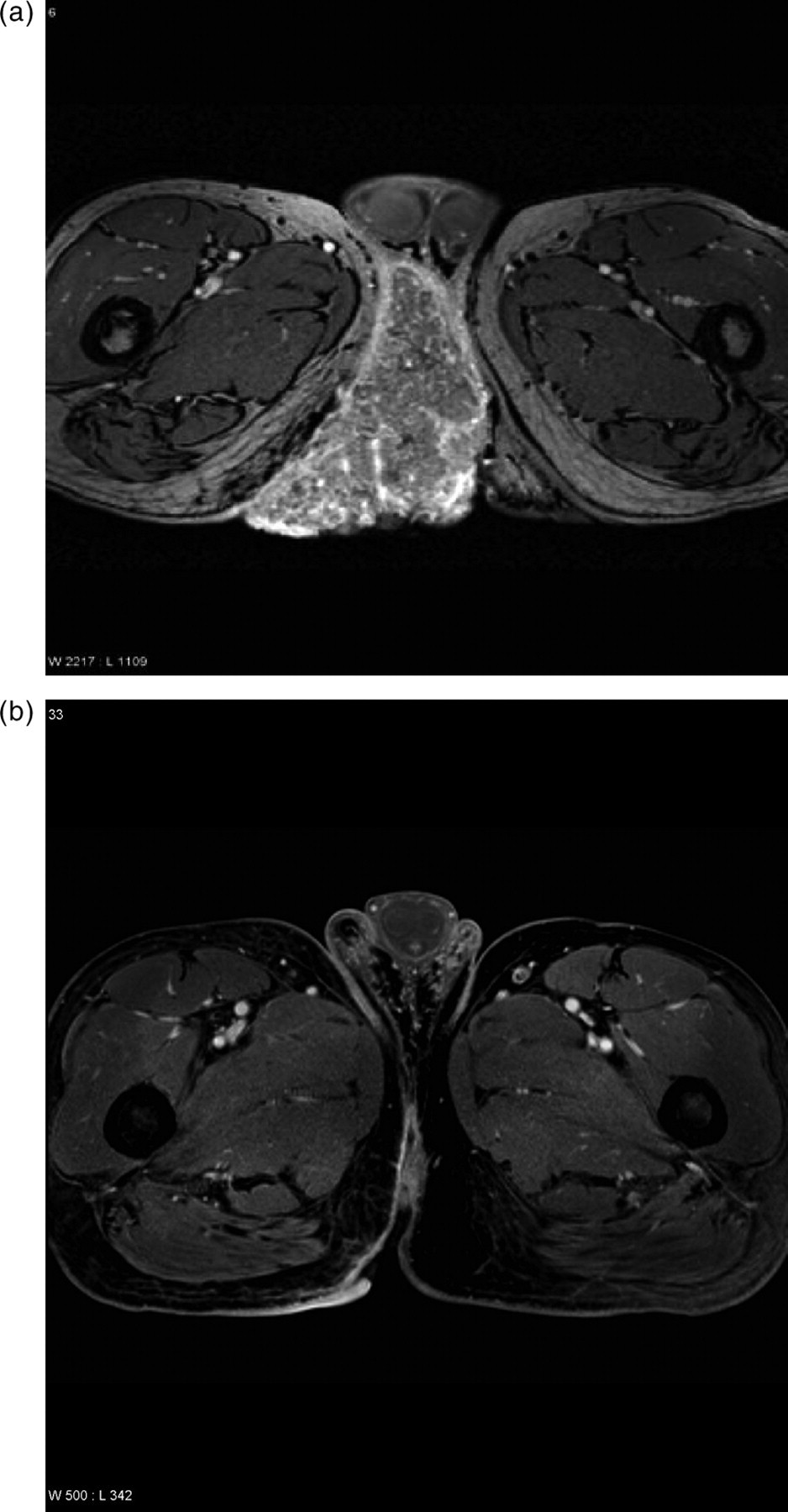
Magnetic resonance imaging images before (a) and after (b) chemo-radiotherapy
The diagnosis and potential treatments were discussed at a Multidisciplinary Team Meeting. Abdominoperineal (AP) resection was considered, but the risk of incomplete excision with residual disease was thought to be high. It was therefore decided to perform a defunctioning sigmoid colostomy followed by chemo-radiotherapy with the aim that if sufficient tumour regression was achieved then radical surgical excision might be possible.
He underwent laparascopic formation of sigmoid colostomy within the next few days and chemo-radiotherapy was commenced two weeks later. He received two cycles of neoadjuvant cisplatin 80 mg/m2 day on day 1 with 5-fluoruracil (5-FU) 800 mg/m2 on days 2–5 at three weekly intervals followed by chemo-radiotherapy using the same chemotherapy regimen on days 1–5 and days 29–33 combined with 50 Gy in 25 fractions using a two-phase technique using parallel opposed fields.
There was a dramatic response to treatment which was confirmed by a repeat magnetic resonance imaging scan. This showed complete resolution of the tumour with only a small fistula on the right but no other disease in the pelvis. A repeat EUA showed an area of ulceration secondary to radiation damage but no recurrence of warts. Biopsies showed focal ulceration of the epithelium but no evidence of either HPV or AIN.
It was therefore felt that further surgery was not needed at that stage, but that he should be kept under close review. Thirty-four months following completion of chemo-radiotherapy he remains well with no evidence of disease recurrence.
DISCUSSION
A Buschke–Lowenstein tumour or giant condyloma acuminatum is a rare variant of HPV infection affecting the external genitalia. Buschke and Lowenstein first described a lesion involving the penis in 1925 1 and it has since been described in the perineum, anus and rectum. HPV subtypes 6 and 11 are most commonly associated 2 and although they are generally regarded as a low-risk types, Buschke–Lowenstein tumours are invasively growing verrucous genital tumours and are clinically regarded as malignant. 3 It is highly aggressive with the propensity for recurrences and malignant transformation, but distant metastases have not been reported.
Local surgical excision has been widely described, but a review of 42 cases showed that 80% of patients who were initially treated with radical surgery developed recurrences. Median time to first recurrence was 10 months and patients with recurrences had an average disease duration of 9.6 years, emphasizing the need for long-term follow-up. 4 There have also been case reports of treatment with systemic chemotherapy, 5 CO2 laser therapy and interferon alpha therapy, 6,7 CO2 laser therapy and imiquimod, 8 and radiotherapy alone, 9 but a preferred option has not been clearly defined. There have been reports of the use of chemo-radiotherapy in cases of Buschke–Lowenstein tumours containing squamous cell carcinoma 10–12 and subsequently Tytherleigh et al. 13 have described the treatment of two cases of Buschke–Lowenstein tumour with combined surgery and chemoradiation.
This case highlights the need for adequate biopsy of any chronic anogenital lesion that does not respond to simple therapies. It also illustrates the diagnostic and therapeutic challenges encountered when managing a patient with such a lesion in the absence of any proven treatment modality. A multidisciplinary approach is important in such cases in order to initiate prompt and appropriate treatment and achieve optimal outcomes. Careful consideration was given to the use of chemo-radiotherapy in a patient with a lesion without evidence of malignant transformation. Although mitomycin C and 5-FU is considered the standard of care for invasive squamous cell carcinoma of the anus, we chose the option of cisplatin and 5-FU as it was likely to be less myelosupressive in a locally invasive tumour without metasases.
This patient with previous disease recurrence demonstrated an excellent response to chemo-radiotherapy without the need for extensive surgery, and we suggest that chemo-radiotherapy be evaluated as the optimal primary therapy for the Buschke–Lowenstein tumour.