
Abstract
There is no evidence that antiretroviral therapy (ART) alone may result in complete remission of aggressive non-Hodgkin's lymphomas even though it improves the overall prognosis. We report a case in which early diffuse large B-cell lymphoma regressed completely after ART alone, raising the possibility that this may be sufficient therapy in selected cases.
Much of the focus on the impact of antiretroviral therapy (ART) on HIV-related lymphomas has been on epidemiology and prognosis when used together with chemotherapy. 1,2 The available literature is silent on whether the use of ART alone can bring about complete remission in diffuse large B-cell lymphomas (DLBCLs). Anthracycline-based regimens such as cyclophosphamide, doxorubicin, vincristine and prednisolone (CHOP) remain the mainstay of treatment. This is probably because they antedated ART, which was introduced as ‘add-on’ therapy. Unfortunately, these regimens and antiretroviral drugs have overlapping toxicities, particularly haematological and neurological. These two systems are also commonly affected in HIV infection. The use of ART alone in early non-Hodgkin's lymphoma may ameliorate these problems and reduce the cost of treatment, a critical consideration in resource-limited settings.
CASE REPORT
A 43-year-old man was referred to the outpatients' clinic with a three-week history of severe epigastric pain, unresponsive to analgesia or ranitidine. There were no other significant symptoms. He had never been tested for HIV. On physical examination he had greying of nails but no lymphadenopathy and no other significant findings. Endoscopy revealed several papular lesions with central umbilication on the greater curvature of the stomach, and multiple biopsies were taken.
An HIV-1 test was positive and his CD4 count was 69 cells/mm3 but a viral load was not done. The gastric biopsies showed a DLBCL, germinal centre subtype (Figures 1a and 1b). The tumour cells were positive for antibodies to CD20 (Figure 2a), and CD10; staining for B-cell lymphoma 6 protein (bcl-6), multiple myeloma oncogene-1, bcl-2, CD3 and Epstein-Barr encoded RNAs were negative. Mindbomb homolog 1 (MIB1) showed a proliferation fraction of over 95 % (Figure 2b). The large size of the tumour cells together with the nuclear pleomorphism, frequent mitotic figures and the high MIB1 percentage all indicated a high-grade lymphoma with aggressive histological features. Staging investigations included an ultrasound scan of the abdomen and a chest X-ray: both of these were normal, suggesting a stage 1E tumour (a tumour still limited to the gastric wall by Ann Arbor classification).
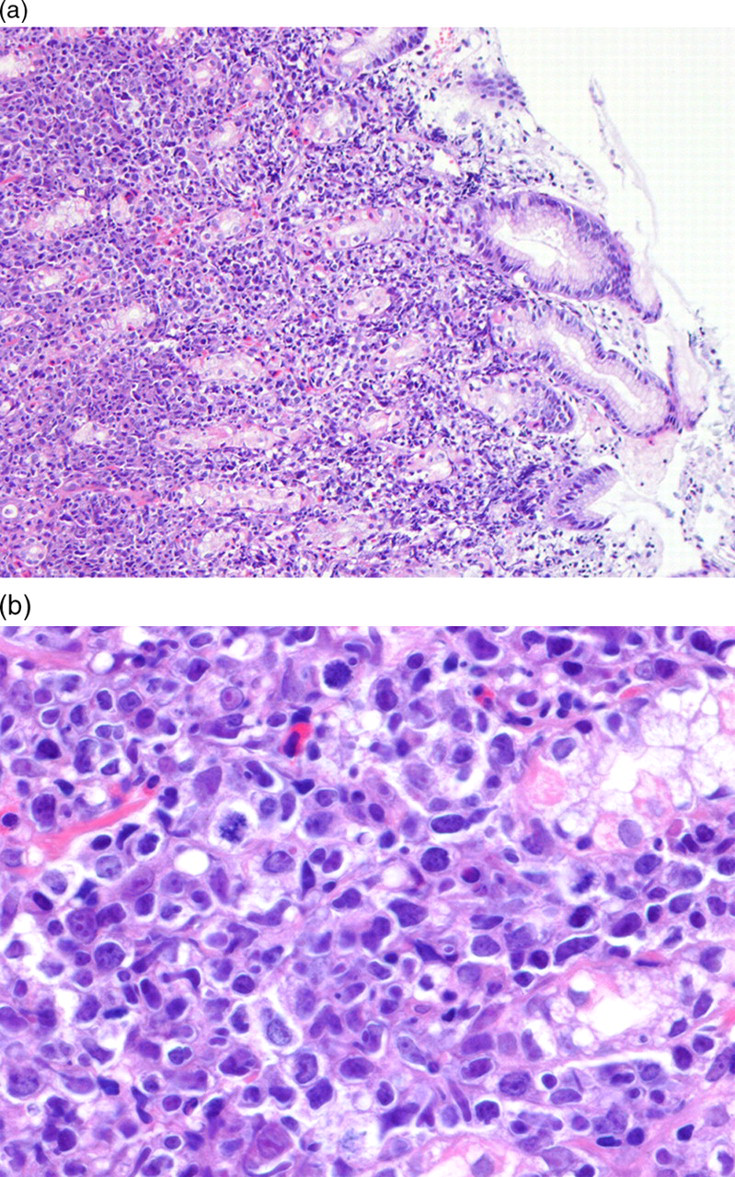
(a) Low-power photomicrograph of superficial gastric mucosa showing lamina propria infiltration by atypical lymphoid cells. Haematoxylin and eosin stain; ×50 original magnification. (b) High-power photomicrograph of gastric mucosa showing large pleomorphic lymphoid cells. Haematoxylin and eosin stain; ×400 original magnification

(a) CD20 immunostaining of tumour cells indicating a B-cell lineage. CD20; ×400 original magnification. (b) Mindbomb homolog 1 (MIB1) immunostaining showing the high proliferation index of the tumour cells. MIB1; ×400 original magnification
Due to unavailability of chemotherapy, the patient was commenced on an antiretroviral regimen of stavudine, lamivudine and nevirapine with informed consent. At review after one month of ART the abdominal pain had resolved and after four months the CD4+ count was 158 cells/mm3. At eight months, the patient remained asymptomatic and a repeat endoscopy showed that the papular lesions had completely disappeared. The multiple biopsies were repeated and there was no histological evidence of residual tumour. One year after initiating ART the patient remains well and he has been scheduled for regular endoscopic surveillance.
DISCUSSION
This case highlights the potential of ART as the sole treatment modality in early stage HIV-related lymphomas. While this may never be subject to a formal randomized controlled trial because of ethical considerations, it provides an option when conventional regimens are not available or not feasible. DLBCL in the setting of HIV are traditionally managed using CHOP and more recently the addition of rituximab to this regimen has been shown to be safe and feasible. 3
The use of ART alone would also be safer and cheaper if proven to be effective as appears to be the case here. Similar cases have already been reported in low-grade mucosa-associated lymphomas but these are much less aggressive tumours, 4,5 with clear infectious aetiologies. 6 There has been one other report of DLBCL regressing on ART alone but this patient still underwent chemotherapy at six weeks despite initial evidence of regression. 6 Therefore, this is the first reported case where long-term remission of an aggressive DLBCL was obtained with the use of ART alone.
Staging could have been improved by a bone marrow aspirate and biopsy, endoscopic ultrasound scan, computed tomography scanning and fluorodeoxyglucose-positron emission tomography. However, our criteria for response were exacting, as they included resolution of symptoms, resolution of the gross endoscopic appearances and absence of histopathological evidence of lymphoma.
A word of caution is that this approach may not be universally applicable, as our patient had fairly localized disease. Furthermore, identification of patients with early disease may be complicated by lack of extensive investigations available in resource-limited settings. Nevertheless, the approach warrants consideration because of its cost-effectiveness. This is an important issue in low resource countries where both availability and affordability of chemotherapy regimens is problematic and HIV-infected patients are often debilitated, rendering them much less able to withstand the rigours of chemotherapy, and they have little access to pre- and postchemotherapy supportive care.
Footnotes
ACKNOWLEDGEMENTS
The clinical contribution of Prof I T Gangaidzo and Prof K Jonsson who performed the pre- and post-treatment endoscopies respectively is acknowledged. We thank Prof R F Miller for his invaluable comments and support.