
Abstract
Genital herpes is one of the most common sexually transmitted infections worldwide. We established a web-based survey to determine risk for genital herpes and encourage people to attend for herpes simplex virus testing. A survey was established on the Australian Herpes Management Forum (AHMF) website, consisting of 16 demographic and sexual health-related questions. Each question carried a numerical risk-weighting based on epidemiological data; the higher the overall score, the greater the risk of herpes. To determine how representative our sample was in relation to age and sex, we compared our survey with Australian Census data. Between October 2006 and August 2007 there were 5572 responses, 4358 (92%) were Australian. Compared with the Australian population, the survey population had a higher proportion of individuals aged less than 34 years, and a lower population over 55. Six hundred and eighty-six (13.8%) were classified as low risk, 2558 (51.6%) as medium risk and 1710 (34.5%) as high risk of having acquired genital herpes. In total, 39% reported four or fewer, and 38% reported 10 or more, sex partners in their lifetime. A large number of individuals participated in this survey, confirming that the Internet is a useful tool for health promotion for genital herpes.
INTRODUCTION
Genital herpes is one of the most common sexually transmitted infections (STIs) throughout the world. In Australia, a recent population-based survey revealed that 16% of women and 8% of men over the age of 25 years had antibodies to herpes simplex virus (HSV)-2 infection. 1 The majority of people infected with HSV-2 are unaware that they are infected, either because they have no symptoms or they have mild, unrecognized symptoms. 2 Until an effective vaccine is available, control of genital herpes will rely on avoidance of sex during outbreaks, the use of condoms and the use of antiviral drugs to reduce the risk of transmission. 3,4 However, for such strategies to be effective, infected individuals will need to know that they are infected. Consequently, it has been suggested that a type-specific serology would be a useful tool for screening populations for HSV-2 infection. 5 However, the benefits of such a strategy have been contested. 6
An additional problem is that many individuals who may have been exposed to HSV-2 may not consider themselves to be at risk. With the increasing availability of web-based technology for use as information and education tools, we decided to establish a web-based survey tool to determine risk for genital herpes and encourage ‘high-risk’ people to attend for HSV testing, and to allow for the collection of data over wide areas.
METHODS
A web-based genital herpes risk assessment quiz was set-up on the Australian Herpes Management Forum (AHMF) website. 7 The quiz was based on epidemiological data derived from a national population-based survey 1 with additional information from other epidemiological surveys conducted in other parts of the world. 8–15 The quiz consisted of 16 questions, nine of which were primary and seven optional. Each question carried a numerical weighting, the higher the overall score, the greater the risk of herpes. The first question related to whether the person was living in Australia or another country. Although the survey was primarily directed at individuals from Australia, we were unable to control access from outside of the country and because Australia has a relatively low HSV-2 prevalence rate, we graded Australia as 1 and other countries as 2. Age was graded as follows: individuals below the age of 16 years were graded as 0; 17–24 as 1; 25–34 as 2 and 35–44 as 3. All those above the age of 45 years were graded 4. The reason for not increasing the grading according to increasing age above 45 years was that in Australia the serological survey showed that there was a plateauing effect in those above the age of 45 years. 1 In keeping with studies in Australia and internationally, women were graded higher than men. 1 In addition, the number of sexual partners, whether a partner had genital herpes and failure to use condoms all ranked higher, as did symptoms that could be attributable to genital herpes.
The optional questions related mainly to marital status, the duration of relationships, educational levels, occupation and income. These were all ungraded. However, we did grade two additional questions. One related to whether they had sex with someone other than their regular partner, which received an increased grading, and the other related to whether the individual was an Aboriginal or Torres Strait Islander, which also received an increased grading based on the population-based serological surveys. Scores for each question were then added up and individuals were given a risk score of low risk, medium risk or high risk for having acquired genital herpes. In order to determine how representative our sample was in relation to the age, sex and indigenous status of the overall population in Australia, we compared the age of the survey population with that of the general population using data from the Australian 2006 Census. 16 This is a method that has been applied in other Internet-based studies. 17
All responses were recorded and analysed using SPSS 15. 18 Incomplete responses were examined and those with data missing of the type used to calculate scores were not included in the analysis. Those that merely had demographic data missing (which was not used to calculate scores) were still included in the final analysis. When performing analysis on different subgroups, account was first taken of the design weights of the study, for example, when comparing men and women, the extra weighting for women was first cancelled out. Participants were asked to note their postcode.
Before we went online, we ran a number of scenarios to determine whether the risk scoring was adequate. The original coding was low risk 0–17, medium risk 18–24 and high risk 25 or above. However, the scenarios revealed that the majority of individuals ranked either high or low risk, and there were very few who fell in the medium result. The second coding graded the risks low 0–17, medium risk as 18–30 and high risk as 31 or over. However, in this scenario, most individuals fell in the low and medium risk categories. The final coding was low risk 0–17, medium risk 18–25 and high risk 25 plus. This seemed to give the best differential between the various risk categories and was the final model that was decided upon.
In order to determine whether the sexual behaviour data were representative, we compared the study data in relation to the lifetime number of sexual partners to similar data derived from the Australian Study of Health and Relationships (ASHR), a large, telephone-based, representative study of sexual behaviour in Australia. 19
All individuals who completed the survey were offered a printout with their individual risk assessment and all were advised to see their health-care provider to discuss the results. Consent for the study was obtained from the Human Research Ethics Committee (HREC) Sydney West Area Health Service (Westmead Campus).
RESULTS
Between the 6 October 2006 and the 31 August 2007 there were 5572 responses to the survey. However, 618 of these were incomplete and could not be included in the analysis, leaving 4954 valid surveys. A valid survey was one in which all information needed for calculating risk scores was provided. Two thousand eight hundred and twenty-five (57%) were men, 2129 (43%) were women and 4358 (92%) were Australian. The demographic characteristics of the survey participants can be seen in Table 1. Of the 4358 Australian participants, 89 (2.04%) reported that they were Aboriginal or Torres Straight Islander (cf. the general population where 2.3% were ATSI in the 2006 Census). 16 Figure 1 shows an age comparison between our sample and the general Australian population based on the 2006 Australian Census data. 16 The survey population had a higher proportion of individuals less than 34 years of age, whereas the general population had far more who were over 55 years of age.
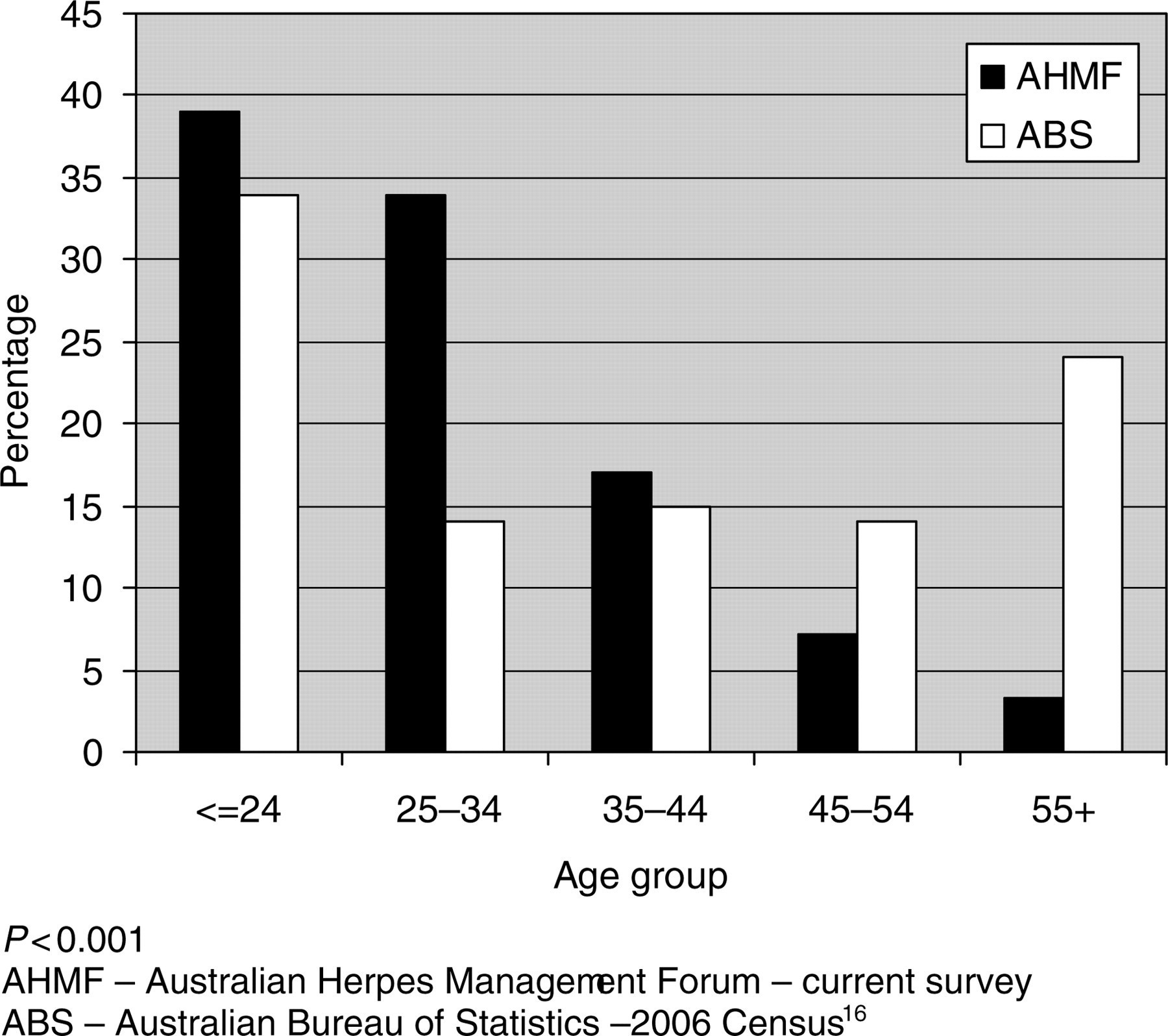
Age groups comparing participants in the survey with those in the general Australian population based on the 2006 Australia census
Demographic characteristics of survey participants (n = 4954)
*Australian participants only
†Technical and further education
‡Remoteness/Accessibility Index of Australia
Six hundred and eighty-six (13.8%) of the participants were classified as low risk, 2558 (51.6%) as medium risk and 1710 (34.5%) as high risk of having acquired genital herpes and the distribution of risk scores can be seen in Figure 2.
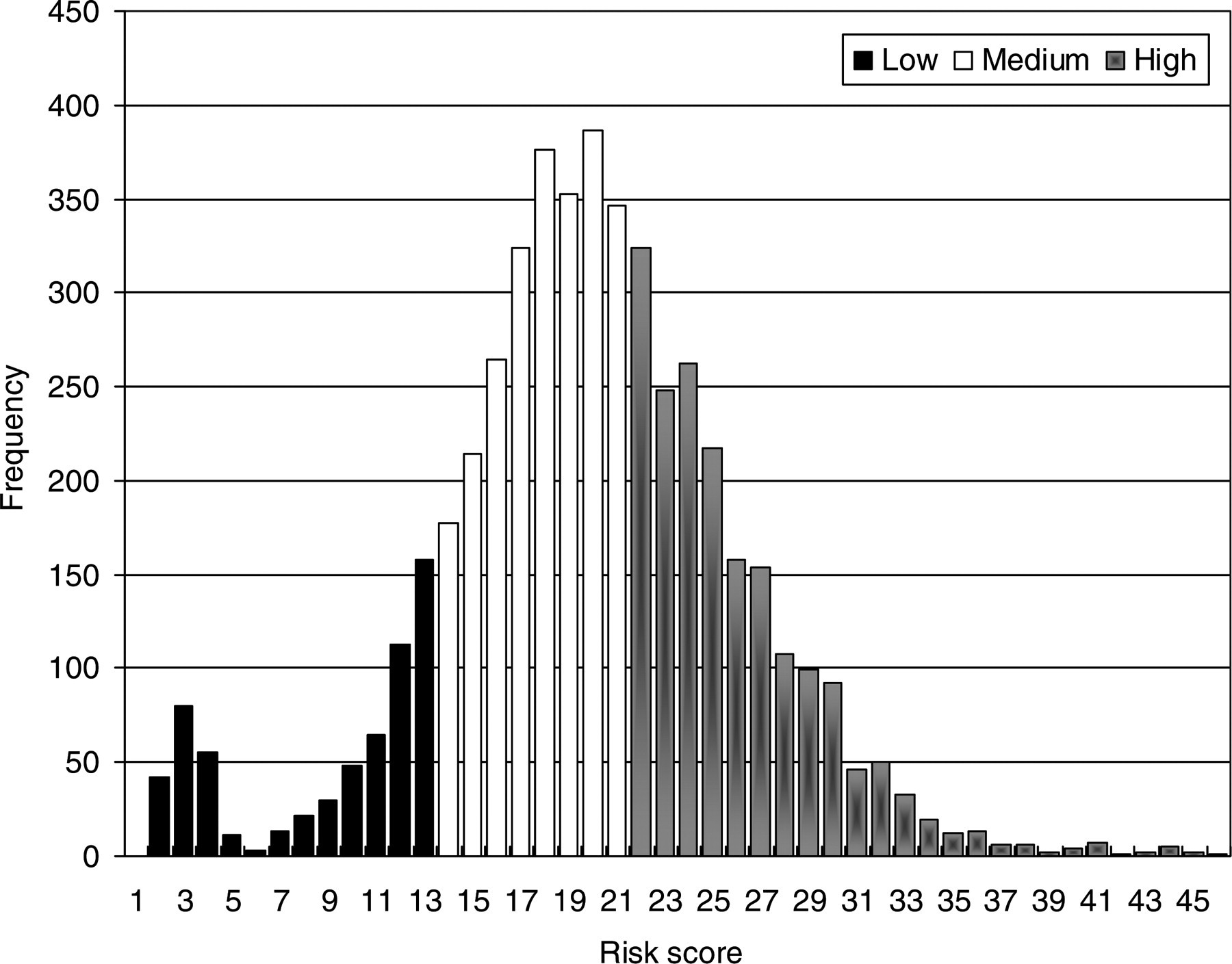
Distribution of risk scores
The sexual behaviour of participants is shown in Table 2. Thirty-nine percent of participants reported four or fewer sex partners in their lifetime and 38% reported 10 or more partners. Twenty-three percent never used condoms and 12% had had sex with someone known to have herpes.
Sexual practices of survey participants
*Number of participants was 4954; however, for all variables other than lifetime number of sex partners, the 196 individuals who said that they had no sexual partner were excluded as none of these answered any of the other sex-related questions
We compared the number of sexual partners in the survey population with data derived from the ASHR study (Figures 3 and 4). There were a number of statistically significant differences between the current survey and the data derived from ASHR. In this survey, there were a larger proportion of women who reported 2–9 sex partners in their lifetime than in the ASHR survey (50.8% versus 42.4%) and a smaller percentage with 10 or more sex partners in their lifetime (31.7% versus 32.7%).

Lifetime number of opposite-sex partners in women comparing participants in the survey with those from the Australian Study of Health and Relationships
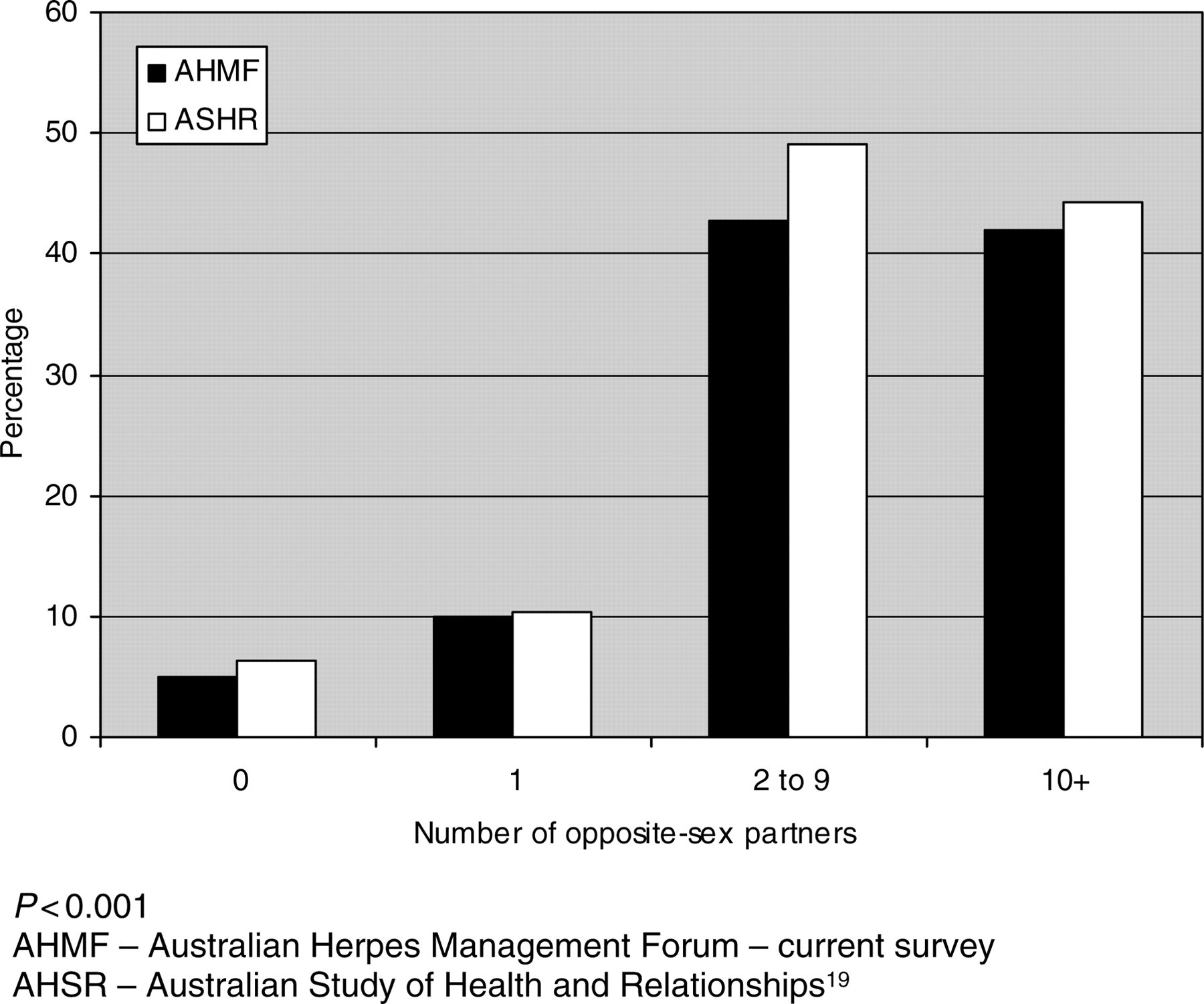
Lifetime number of opposite-sex partners in men comparing participants in the survey with those from the Australian Study of Health and Relationships
The symptoms and signs suggestive of genital herpes were compared in male and female participants (Table 3). Male participants were more likely than female participants to report blisters in the genital area (27% versus 24.4%, P < 0.05) and tingling in the genital area thighs or buttocks (27% versus 22% P < 0.001), whereas females were more likely than males to report genital itching (64.2% versus 51.9%) and genital burning (29.1% versus 19.3%), P < 0.001 for both.
Symptoms or signs suggestive of genital herpes comparing men and women
DISCUSSION
A large number of individuals participated in this risk survey, suggesting that using the Internet may be a useful strategy for health promotion for genital herpes and encouraging individuals who may not otherwise seek advice or health care, to be assessed for risk and to be directed to a health-care provider. In a large telephone survey in the USA, almost half of the participants who perceived themselves to be at risk of contracting herpes had modified their behaviour as a result of this perception, and among those never married, 60% stated that they were willing to modify their lives to avoid herpes. 20 There are implications for public health resource planning resulting from self-identifying high-risk individuals who may be encouraged to be tested as a result of increased awareness of their risk, including increased demand for herpes type-specific serology and consequent counselling and advice and possible treatment for those being tested. A cross-sectional study from a genitourinary (GU) medicine clinic in the UK found that the vast majority of attendees not only wanted to be tested for herpes but also accepted the test when offered. 21 However, the value of screening and, in particular, the use of type-specific serology remains contentious. 5,6 The benefit of self-selecting high-risk individuals seeking testing is that resources are utilized by those most in need, thus improving cost-effectiveness.
There are other advantages of Internet health promotion, including access to a wide and diverse population and the ability to access marginalized or minority groups. Internet-based health promotion, including sex education and information about STIs, has been shown to be acceptable to men who have sex with men (MSM), 22 school children in China 23 and adolescents. 24 A previous study of individuals with ‘stigmatized illnesses’, including herpes, concluded that individuals with such illness were more likely to use the Internet for health information than those without such illness. 25 However, by definition, Internet surveys restrict the sample population to those who have access to the Internet. Due to the sensitive nature of an STI-based survey, this subset is likely to be further restricted to those who have Internet access at home. In Australia, the 2006 Census showed that 63% of dwellings had access to the Internet 16 and this proportion has probably increased in the last two years. In addition, there may be cultural or other limitations on Internet use.
Internet-based educational resources and health promotion materials for genital herpes are widely available, 7,26–30 However, a meta-analysis of health promotion material available on the worldwide web has shown that readability, reliability, and accuracy vary enormously. 22,31 Providing guidance to the population about reliability and accuracy of Internet resources remains challenging, particularly as inaccurate information and even inappropriate access to incorrect treatments may lead to individuals being unnecessarily treated or believing that they may not require treatment when the opposite may be true. 32
The major strength of this study was the large number of participants. One limitation could be that the population had some demographic and sexual differences when compared with the broader Australian community. However, these differences were small and reflect the fact the genital herpes is considered more of a problem in younger and more sexually active individuals.
The gathering of information via online surveys provides an opportunity to educate and, at the same time, to disseminate and collect information from a broad base and to expose a larger audience than many other educational platforms in the most cost-effective way.