
Abstract
Pneumocystis jirovecii pneumonia (PCP) prophylaxis may be discontinued when CD4 is ≥200 cells/mm3 for three months in response to highly active antiretroviral therapy (HAART). Unlike CD4, the total lymphocyte count (TLC) is inexpensive and widely available in resource-constrained countries. Paired TLC and CD4 values of HIV-infected patients attending an HIV clinic from 1998 to 2005 were analysed by Spearman's correlation. The sensitivity, specificity, positive predictive value, negative predictive value and receiver operating characteristics (ROC) using TLC cut-off points between ≥1400 and ≥2000 cells/mm3 to predict CD4 ≥200 cells/mm3 were calculated. Next, a cohort of patients who had a TLC ≤ 1200 cells/mm3 and subsequently achieved various TLC cut-off points sustained over three months while receiving HAART was identified. Subjects with subsequent CD4 ≥200 cells/mm3 in response to HAART were considered to have negligible risk for PCP. There was significant correlation between TLC and CD4 in 46,250 observations from 4307 individuals (r = 0.695, P ≤ 0.001). The area under the ROC curve was 0.85 (95% CI = 0.85–0.86). In the historical cohort analysis, 85% and 70% of subjects who achieved TLC ≥ 2000 cells/mm3 and ≥1400, respectively, had a corresponding CD4 ≥ 200 cells/mm3. A sustained rise in TLC in response to HAART may potentially serve as a criterion for discontinuing PCP prophylaxis in resource-constrained countries.
Introduction
At the end of 2007, there were an estimated 33 million people living with HIV (PLWH) in the world, with 95% living in resource-constrained countries. 1 Resource-constrained countries are increasingly offering highly active antiretroviral therapy (HAART). The initiation of HAART and opportunistic infection (OI) prophylaxis, the monitoring of treatment response, and the discontinuation of OI prophylaxis are based largely upon the CD4 lymphocyte count in developed countries.
Studies in developed countries have demonstrated the safety of discontinuing Pneumocystis jirovecii pneumonia (PCP) prophylaxis when the CD4 lymphocyte count is ≥200 cells/mm3 for at least three months in response to HAART.2,3 In two studies from India and Thailand no subjects developed PCP or cerebral toxoplasmosis when co-trimoxazole prophylaxis was discontinued at similar CD4 lymphocyte thresholds.4,5 The WHO recommends discontinuing co-trimoxazole when the CD4 increases to ≥200 or ≥350 cells/mm3 for six months if prophylaxis is mainly to prevent PCP and toxoplasmosis, or where malaria and bacterial infections are prevalent, respectively. 6
Despite the central role of CD4 lymphocyte testing in treatment algorithms in the developed world, the cost of routine testing in many resource-constrained countries may be prohibitive. 7 However, because the total lymphocyte count (TLC) is inexpensive and widely available, 8 its use as a low-cost substitute for CD4 has been explored.9–11
The main goal of this study was to model the risk of developing PCP after hypothetical PCP prophylaxis discontinuation based upon reaching and sustaining various TLC thresholds in response to HAART.
Methods
Montefiore Medical Center (MMC) is an academic teaching hospital in the Bronx, New York. The MMC Infectious Diseases Clinic provides comprehensive medical care to over 2500 persons living with HIV/AIDS. CD4 lymphocyte counts and TLCs for these patients are performed in the MMC Clinical Laboratory. Between 1998 and 2005, all laboratory results from the MMC Clinical Laboratory were recorded in the hospital's clinical information system (CIS). The hospital maintains a secure replicate of the CIS data environment for quality improvement and research purposes. This data replicate was interrogated in order to produce a table of all paired CD4 and TLC measurements drawn from ID Clinic patients during that eight-year time period. CD4 cell count (FACscan, Becton Dickenson, San Jose, CA, USA) and TLC (Sysmex automated hematology analyzer; Sysmex America Inc, Mundelein, IL, USA) obtained on the same day were considered as paired. These data were linked to demographic information that was also available in the database. In the event that further information was required, especially data related to antiretroviral treatment history, paper charts were reviewed and abstracted. Data were stored in a secure database, and all analyses were completed using the SPSS for Windows V14.0 software package (SPSS version 14.0, Chicago, IL, USA). All aspects of the study were approved by the MMC Institutional Review Board. The present study includes two separate analyses.
Analysis I: Correlation of paired TLC/CD4 measurements and evaluation of TLC cut-off values
The association between CD4 lymphocyte count and TLC was determined by Spearman's correlation coefficient. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for TLC cut-off points between ≥1400 and ≥2000 cells/mm3 in 100 cells/mm3 increments to predict CD4 ≥200 cells/mm3 were calculated for the entire group. The relationship between sensitivity and specificity was examined using receiver operating characteristic (ROC) curves and the area under the ROC curve (AUC). The 95% confidence intervals (CIs) of the AUC were used to compare diagnostic accuracy among subgroups.
Analysis II: Estimation of PCP risk after hypothetical discontinuation of PCP prophylaxis
The goal of the second analysis was to model the risk of developing PCP after hypothetical PCP prophylaxis discontinuation based on achieving various TLC thresholds, using a historical prospective cohort design. The study population from the first analysis was screened for eligibility and included if they met the criterion for PCP prophylaxis any time in the past, defined by a TLC < 1200 cells/mm3. There are currently no WHO recommended TLC-based thresholds to initiate PCP prophylaxis. However, this criterion was chosen for the study because initiation of HAART is recommended in those with WHO clinical stage 2 and TLC < 1200 cells/mm3. 12 Secondly, subjects were eligible if they subsequently had a sustained immune improvement in response to HAART, defined by having all TLCs, with a minimum of two measurements, greater or equal to a specified TLC threshold for a period of at least three months. Separate, but overlapping, cohorts were created for TLC thresholds starting from ≥1400 cells/mm3 and increasing by increments of 100 to ≥2000 cells/mm3. For example, a patient having a TLC of 1000 cells/mm3 on 1 January 2003, a TLC of 1500 cells/mm3 on 1 March 2003 and a TLC of 1700 cells/mm3 on 1 July 2003 would be included in both the 1400 and 1500 cells/mm3 cohorts, but not in the higher TLC cohorts (unless subsequent TLC measures qualified him/her for inclusion). Receipt of HAART was confirmed by review of the clinic record. HAART was defined as receipt of at least three antiretroviral drugs, excluding ritonavir used as a pharmacological booster. The primary endpoint in each cohort was the occurrence of risk of developing PCP, defined as CD4 lymphocyte count <200 cells/mm3, after hypothetical PCP prophylaxis discontinuation. According to the model, these subjects would have been mistakenly taken off of PCP prophylaxis, as a result of relying on TLC as a surrogate marker. Such patients were considered ‘at risk’ until either the CD4 increased to 200 cells/mm3 or their TLC decreased to below the prespecified TLC threshold (at which time the model would call for resumption of PCP prophylaxis) and the median duration of time at-risk was estimated by Kaplan-Meier analysis for each cohort. For at-risk subjects in whom the CD4 later increased to ≥ 200 cells/mm3, a linear increase was assumed, and the time at which CD4 crossed the 200 cells/mm3 threshold was used for calculating the duration of risk. Stratified analyses were also conducted to determine any differences by gender or race. The number of hypothetical PCP cases per 100 patient-years in each cohort was estimated by multiplying the estimated time at risk with published PCP incidence rates from previous epidemiological studies of at-risk PLWH.
Results
Analysis I
There were 46,250 paired CD4 lymphocyte and TLC from 4307 HIV-infected individuals between 1998 and 2005. The median age was 40 years with an interquartile range (IQR) of 34–47 years. Fifty-seven per cent were men, 51% Hispanic, 40% Black and 5% White. Median CD4 was 342 cells/mm3 (IQR 182–542 cells/mm3) and the median TLC was 1700 cells/mm3 (IQR 1200–2300 cells/mm3).
Bivariate analyses demonstrated a high degree of correlation between TLC and CD4 (Spearman's rho = 0.695, P < 0.001). The sensitivity, specificity, PPV and NPV for various TLC cut-off points as predictors of CD4 ≥200 cells/mm3 are listed in Table 1. As expected, sensitivity and NPV increased as the cut-off point decreased, whereas specificity and PPV increased as the cut-off point increased.
Performance characteristics of TLC cut-off points as predictors of CD4 ≥ 200 cells/mm3
TLC = total lymphocyte count; PPV = positive predictive value; NPV = negative predictive value
The AUC was 0.85 (95% CI = 0.85–0.86). In subgroup analyses, there were small but statistically significant differences in AUC between women 0.87 (95% CI = 0.87–0.88) and men 0.84 (95% CI = 0.83–0.84), P < 0.001; Hispanic 0.85 (95% CI = 0.84–0.86) and White 0.82 (95% CI = 0.80–0.84), P = 0.003; and Black 0.86 (95% CI = 0.85–0.87) and White, P < 0.001.
Analysis II
Table 2 summarizes the results of the historical prospective cohort analysis. The number of subjects, percentage with concurrent CD4 lymphocyte < 200 cells/mm3 and median days of risk for PCP by Kaplan-Meier estimate are shown by TLC threshold. HAART regimens consisted of two nucleoside reverse transcriptase inhibitors (NRTIs) plus a protease inhibitor (PI) (52%); a non-nucleoside reverse transcriptase inhibitor (NNRTI) plus two NRTIs (34%); three NRTIs (11%); two NRTIs, a PI and an NNRTI (2%); or undetermined (1%). The median concurrent CD4 lymphocyte count after reaching TLC thresholds within each cohort was well over 300 cells/ mm3. As expected, the percentage with concurrent CD4 lymphocytes < 200 cells/mm3 in each cohort decreased as TLC thresholds increased. That is, the risk for PCP decreased as the TLC thresholds required for discontinuing PCP prophylaxis increased. For subjects at risk, i.e. those with concurrent CD4 < 200 cells/mm3, the median concurrent CD4 after reaching TLC thresholds within each cohort ranged between 120 and 152, and the median duration of risk ranged between 102 and 131 days.
Cohort characteristics according to TLC threshold
TLC = total lymphocyte count; PCP = Pneumocystis jirovecii pneumonia
Figure 1 depicts the percentage of subjects at risk for PCP (those with concurrent CD4 lymphocytes < 200 cells/mm3) in the entire cohort, and also according to gender, by TLC cohort. Women had a significantly lower risk for PCP than men at every TLC threshold. There were no differences found between races (not depicted). Table 3 shows the estimated number of PCP cases per 100 person-years (PY) combining known incidence rates from published prospective cohorts of HIV-infected patients with CD4 < 200 cells/mm3 and not on prophylaxis in the United States 13 (18% per PY), Brazil 14 (27.7% per PY), Thailand 15 (18.4% per PY) and South Africa 16 (2.4% per PY) with data from Table 2.
Percentage of subjects with CD4 < 200 cells/mm3. TLC = total lymphocyte count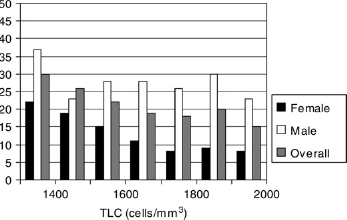
Estimated number of excess PCP cases (per 100 patient-years) according to previously published incidence rates
TLC = total lymphocyte count
Discussion
This is the first study that we are aware of to model the use of TLC for discontinuing PCP prophylaxis in response to HAART-associated immunological improvement. There are many potential benefits of discontinuing co-trimoxazole including avoiding adverse reactions such as rash and anaemia, 17 reducing pill burden, delaying bacterial, 18 and PCP antibiotic resistance, 19 and reducing cost. Despite recent advances in diagnostic technology, the cost of CD4 lymphocyte testing is about US $4–25 per test plus an initial capital cost of US $20,000–35,000, whereas TLC costs approximately US $0.80 per test20,21 and is widely available.
In this study we demonstrate the feasibility of using TLC thresholds to guide the discontinuation of PCP prophylaxis in patients who respond to HAART. The correlation between TLC and CD4 and the sensitivities and specificities at various TLC cut-off points to predict CD4 ≥200 cells/mm3 are similar to studies done in various developing countries.9–11 In this study, the increase in specificity for TLC cut-off points to predict CD4 ≥200 cells/mm3 did not plateau at any of the analysed cut-off points. In the historical prospective cohort analysis, the majority of subjects achieving the TLC thresholds had concurrent CD4 lymphocyte counts ≥200 cells/mm3 in response to HAART. The expected incidence of PCP using a TLC threshold strategy to discontinue PCP prophylaxis in various developing countries was relatively low, ranging from 0.1 to 2.9 cases per 100 PY depending on the TLC threshold selected and the historical reference cohort used to impute incidence rates. Our model likely overestimated the risk of PCP because extremely low CD4 counts, associated with the highest risk, were uncommon in those achieving the specified TLC cut-off points. The expected incidence rate of PCP predictably decreased as TLC thresholds increased.
In subgroup analysis, women had a statistically significant lower risk for PCP than men at every TLC threshold cohort. Women also had a statistically significant larger AUC than men in Analysis I. However, these differences between genders were mathematically trivial and unlikely to be of clinical consequence. There were small differences between races in the ability of TLC to predict CD4, but there was no difference found in the proportion at risk in the historical prospective cohort analysis.
A major limitation of this study was that it did not study a population from a resource-constrained country. Also, while laboratory costs for TLC are lower than CD4 lymphocyte measurement, a TLC-based approach to PCP discontinuation may not necessarily be cost-effective. Due to low sensitivity, there may be missed opportunities to stop prophylaxis and to save on drug costs. Conversely there are potential costs of treating those who develop PCP after inappropriate prophylaxis discontinuation. Additionally, this study did not incorporate other parameters such as haemoglobin, body mass index and WHO clinical staging, which may increase sensitivity and specificity over TLC alone. 22 These weaknesses may be counterbalanced by the large number of paired samples available for analysis and by the enrolment of a racially diverse population.
The TLC may also be influenced by factors other than HIV infection. Relatively common infections such as tuberculosis, 23 malaria 24 and RSV 25 along with medications such as corticosteroids 26 and chemotherapy may decrease the TLC. Conversely, illnesses such as infectious mononucleosis and HTLV-1/2 infection 27 may increase the TLC. This underscores the importance of avoiding immunological testing with TLC or CD4 during acute illnesses.
In summary, PCP prophylaxis discontinuation based on achieving TLC thresholds in response to HAART may be a reasonable strategy for PLWH in resource-constrained settings. Our findings suggest that the risk of PCP is comparatively low for prophylaxis discontinuation strategies in the TLC range that we studied. Careful cost-benefit analyses will be required to determine an optimal TLC cut-off point. Ultimately, clinical trials in resource-constrained areas of the world may be indicated to test the safety and cost-savings of TLC guided OI prophylaxis discontinuation strategies.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Yungtai Lo of the Center for AIDS Research, Montefiore Medical Center for his assistance with the statistical analysis.
This work was supported by the Clinical Core of the Center for AIDS Research at the Albert Einstein College of Medicine and Montefiore Medical Center funded by the National Institutes of Health (NIH AI-51519).