
Abstract
Isolated thrombocytopaenia can occur in 30–60% of HIV-infected patients. The majority of patients with HIV-related immune thrombocytopaenia have only minor submucosal bleeding problems. Cases of subarachnoid haemorrhage and subdural haematoma are very rare and management of such cases is a challenging problem for physicians. We report a rare case of subdural haematoma due to thrombocytopaenia in a 40-year-old HIV-positive man.
Introduction
Thrombocytopaenia can occur independent of other cytopaenias at all stages of HIV infection. Thrombocytopaenia of some degree may occur in 30–60% of HIV-infected patients. 1 Most patients with HIV-related immune thrombocytopaenia have only minor submucosal bleeding characterized by petechiae, ecchymosis and occasional epistaxis. Rarely, patients may have gastrointestinal blood loss. 1 Cases of subdural and subarachnoid haemorrhages due to thrombocytopaenia in HIV are infrequently reported infrequently 2 and management of such cases poses a challenge for physicians. We report a rare case of subdural haematoma due to thrombocytopaenia in a HIV-positive patient.
Case Report
A 40-year-old man was admitted in the emergency room with severe intractable headache and vomiting. The present complaint started 10 days ago with severe headache for which he was treated symptomatically, though he did not respond to routine analgesics. The headache had increased in severity day by day and the patient developed vomiting two days prior to admission. There were no constitutional symptoms. There was no previous history of such episodes and no history of head injury or seizures was reported. The patient had undergone surgery for a hydrocele two years previously. The operation was uneventful, all of the investigations at that time were within normal limits and he was HIV sero-negative. The patient neither smoked, nor drunk alcohol, was married with two children, but did report recent extramartial contacts. He denied a history of sexual contact with other men.
On clinical examination, the patient was conscious, coherent and well-oriented. All his vital signs were within normal limits. The patient was not anaemic and there was no lymphadenopathy or organomegaly. Detailed central nervous system examination revealed no abnormalities and fundoscopic examination was normal. All other systems were normal. There were no active skin, mucosal or genital lesions and all other systems were normal. There were no clinical signs of external or internal bleeding. Routine haematological, biochemical and screening tests for HIV, HBV and HCV were performed, as well as a chest X-ray, abdominal ultrasound and magnetic resonance imaging (MRI) of the brain. Haemogram revealed haemoglobin 13.4 g%, white blood cell count of 7500 cells/mm3, (neutrophils 72%, lymphocytes 27%, eosiniophils 1%) and platelet count 27,000 cells/mm3. His bleeding time was two min 55 s, clotting time five min five s, prothrombin time 14 s and activated partial thromboplastin time 30.7 s. His peripheral smear revealed normocytic normochromic erythropoiesis with thrombocytopaenia. Biochemical tests were normal, as were urine and stool examinations. The patient tested positive for HIV-1 by enzyme-linked immunosorbent assay and this result was confirmed by Western blot test. His CD4 count was 156 cells/ mm3 and plasma HIV-1 RNA was 36,490 copies/mL. He tested negative for hepatitis B and C virus markers. His chest X-ray and abdominal ultrasound were normal, but the MRI of the brain revealed a large, left hemispheric acute subdural haematoma with significant mass effect in the form of midline shift to the right, with subfalcine herniation, compression and attenuation of the left lateral ventricle and effacement of cortical sulci and fissures (Figures 1a and 1b). In view of his stable neurological condition with underlying thrombocytopaenia, the case was managed conservatively without any surgical intervention. He was managed with oral phenytoin 300 mg/ day, oral prednisolone 30 mg/day in tapered doses and five units of platelet transfusions. The patient was started on antiretroviral therapy (ART) with zidovudine, lamivudine and efavirenz. The patient became asymptomatic and was discharged after two weeks. He was asked to continue his ART and report for follow-up every week for the first three months. It was observed that after starting ART, there was an increase in platelet counts every month and the patient remained asymptomatic. MRI of the brain was repeated after three months and was found to be normal with complete resolution of the subdural haematoma (Figure 2a and 2b). During the follow-up period of one year, the patient was asymptomatic. There was four-fold increase in platelet counts.
T1 (a) and T2 (b) weighted magnetic resonance images showing left-sided subdural haematoma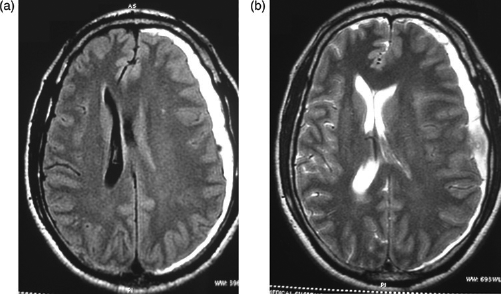
T1 (a) and T2 (b) weighted magnetic resonance images showing complete resolution of subdural haematoma
Discussion
Unlike anaemia and other granulocytopaenia, thrombocytopaenia is not directly correlated with the stage or prognosis of HIV infection. 3 The exact mechanism of HIV-related thrombocytopaenia is not known. The causes of thrombocytopaenia in HIV infection include reduced bone marrow production and both immune and non-immune peripheral destruction of platelets. 1 In the majority of the cases, thrombocytopaenia can lead to only minor bleeding problems in HIV patients. Cases of subarachnoid haemorrhage and subdural haematomas are rarely reported. According to the available data, only one case of spontaneous subarachnoid haemorrhage induced by thrombocytopaenia without any vascular malformations has been reported.
In our case, since there was no history of head injury, MRI studies revealed no vascular abnormalities and laboratory investigations showed isolated thrombocytopaenia, the spontaneous subdural haemorrhage could be due to underlying thrombocytopaenia alone. Another distinct feature of our case was that there were no signs of a bleeding diathesis even though the platelet count was below 30,000 cells/mm3. Management of cases like ours poses a challenging problem for both physicians and neurosurgeons. HIV-infected patients tend to be regarded as poor candidates for surgery because of their immunodeficiency, and thrombocytopaenia adds further to poor prognosis. In general, treatment for HIV-related thrombocytopaenia remains controversial. The use of standard approaches such as corticosteroids and splenectomy are complicated by increased immunosuppression. The response to corticosteroids is generally short-lived. 4 Several studies have reported that an ART regimen containing zidovudine increases platelet counts and corrects thrombocytopaenia in HIV-positive patients.4–6 The mechanism by which zidovudine improves thrombocytopaenia is unclear and seems not to be related to its ART action. 7 Other treatments used for classic immune thrombocytopaenia such as IV gammaglobulin, anti-Rh(D), vincristine, danazol and interferon alpha-2a have all achieved variable success in the HIV-infected patient. 4 We successfully managed our case with a conservative approach and zidovudine-based ART. His subdural haematoma resolved spontaneously with correction of his thrombocytopaenia within three months of ART.
HIV-positive patients with neurological emergencies should be thoroughly investigated and evaluated before any aggressive surgical interventions. As in the present case, such conservative management and specific ART may be beneficial to these patients who may subsequently avoid invasive neurosurgical procedures.