
Abstract
Penicillium marneffei is an opportunistic fungal pathogen in HIV disease. We report the case of a patient with AIDS who presented with general weakness and generalized skin rashes. No specific allergic history or recent medication were reported. The skin lesions disappeared after adequate antifungal therapy. A blood culture obtained from the patient confirmed the presence of P. marneffei, infection which is characterized by cutaneous umbilicated lesions in AIDS patients. We report this case on account of the unusual skin presentation.
INTRODUCTION
Penicillium marneffei is a fungus that has emerged as the third most common opportunistic infection – after extrapulmonary tuberculosis and cryptococcosis – in AIDS patients in southeast Asia. 1–3 The clinical presentations of penicilliosis include fever, lymphadenopathy, hepatosplenomegaly and cutaneous lesions. 3 Approximately 70% of infected patients present with typical skin lesions: papules with central umbilication (resembling molluscum contagiosum), nodules or necrotic lesions. 3,4 However, there have been no reports of patients presenting with a disseminated skin rash caused by systemic P. marneffei infection. Here, we report the case of an AIDS patient who presented with a generalized skin rash, in whom the diagnosis of systemic P. marneffei infection was made.
CASE REPORT
A 42-year-old man who has sex with men presented to our hospital on account of a poor appetite and general weakness that had persisted for five days. On examination, he appeared pale, his body temperature was 36.8°C, pulse rate was 90 beats per minute and blood pressure was 120/80 mmHg. Despite oral candidiasis and generalized skin rash (Figure 1), the physical examination was non-contributory. On admission, his complete blood cell count revealed pancytopenia (haemogloblin: 10.2 g/dL; white blood cell count: 3500 cells/mm3; platelets: 133,000/mm3). The biochemical parameters were normal. Western blot analysis confirmed HIV infection and his CD4 cell count was 15 cells/mm3. Chest radiograph showed bilateral perihilar infiltration. Pneumocystis jiroveci pneumonitis was confirmed by blood and sputum polymerase chain reaction and he received sulphamethoxazole/trimethoprim treatment. Oral candidiasis was treated with oral fluconazole (100 mg daily). We also prescribed levofloxacin for his bilateral pneumonia. However, the persistent skin rashes and fever could not be explained by the identified opportunistic infections until a mould was grown from blood. Intravenous amphotericin B (0.6 mg/kg/day) was commenced for fungaemia. The fever and skin rashes subsided two days after amphotericin B administration. The course of amphotericin B was continued for four weeks after the mould was confirmed as P. marneffei. Thereafter, antiretroviral therapy was initiated and amphotericin B was replaced with oral itraconazole for maintenance treatment of the systemic P. marneffei infection. The patient was discharged and thereafter underwent regular follow-up.
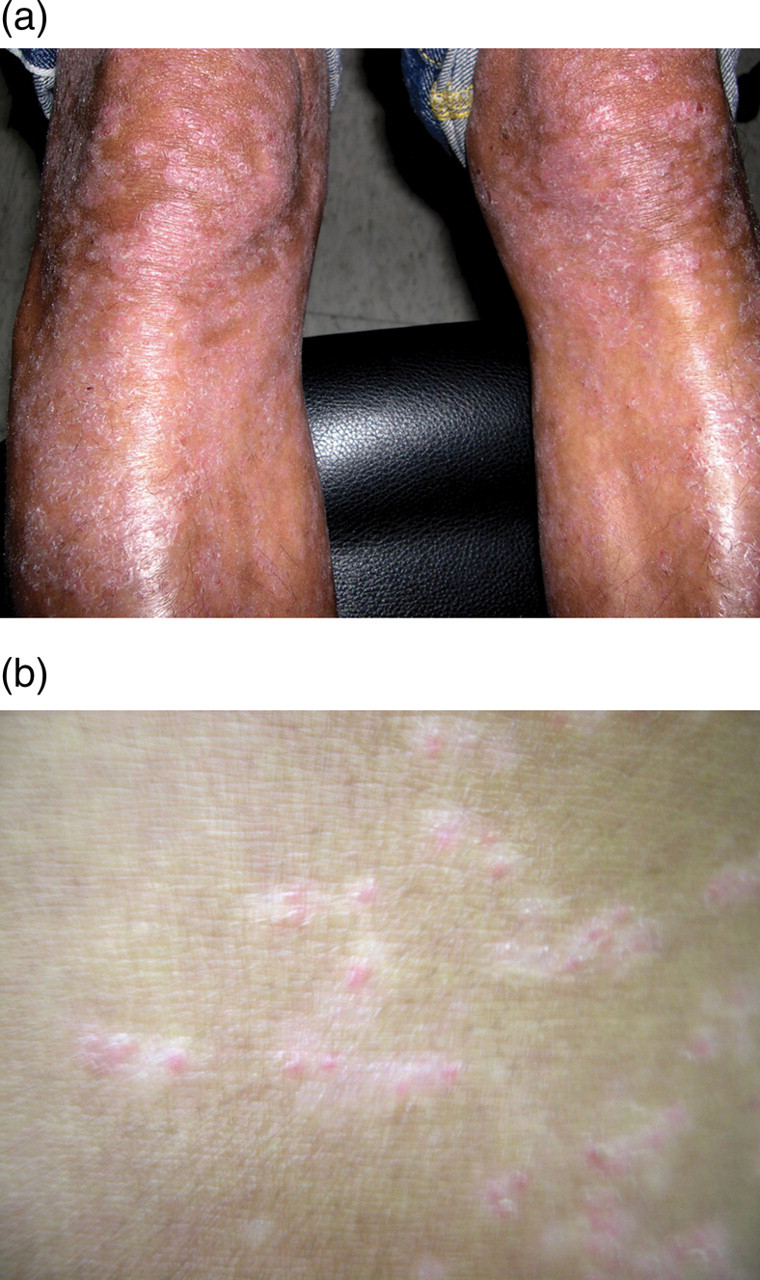
(a) The generalized skin lesions caused by Penicillium marneffei fungaemia. (b) Close-up view of the skin lesions shown in (a)
DISCUSSION
P. marneffei is an important dimorphic fungus that causes life-threatening infection, particularly in immunocompromised patients. P. marneffei was first isolated in 1956 in Vietnam from the bamboo rat Rhizomys sinensis, 1 and the first AIDS patient infected by P. marneffei was described in 1988. 5 It is now the third most common HIV-related opportunistic infection after tuberculosis and cryptococcosis in southeast Asia. 1–3 Areas in which the fungus is endemic include the following: Thailand, Myanmar (Burma), Vietnam, Cambodia, northeastern India, Hong Kong, Taiwan and southern China. 2 However, most reported cases have been from Thailand, with 1173 HIV-infected patients diagnosed at the Chiang May University Hospital from 1991–97. 2 Infection with P. marneffei is acquired by inhalation of conidia from environmental sources such as soil. The clinical presentations include fever, lymphadenopathy, hepatosplenomegaly and skin lesions. Table 1 lists the frequencies of the various presentations. 3 The cutaneous lesions usually appear as papules, nodules or necrotic lesions. These lesions are predominantly located over the face and upper trunk. The characteristic central umbilication of papules resembles molluscum contagiosum.
Clinical features of Penicillium marneffei infection 3
In terms of the treatment of HIV-infected patients with penicilliosis, Supparatpinyo et al. report a case series in which the response to medication with amphotericin B, itraconazole and fluconazole is described. The failure rate (defined as a lack of clinical response, clinical deterioration or persistent fungaemia) was 22.8% for amphotericin B, 25% for itraconazole, 63.6% for fluconazole and 100% for no treatment. 6
To the best of our knowledge, the presentation of disseminated cutaneous rashes in cases of P. marneffei infection has not been previously reported. In advanced AIDS patients who present with generalized skin rashes, opportunistic fungal infection, particularly that of P. marneffei, should be considered when patients reside in endemic areas.