
Abstract
Changes to sexual health clinics have recently been driven by government waiting time targets. However, patients' needs and expectations should be equally important when making service alterations. This study sought to determine what patients valued most when attending an integrated sexual health clinic. During February 2009, 252 patients attending a sexual health clinic in outer London completed an anonymous questionnaire. The questionnaire asked for their views on different aspects of sexual health care. The results showed that the most highly valued aspects of care were confidentiality (18.47% of points allocated) followed by speed of service (13.1%) and rapid test results (12.12%). These aspects were more important than being seen within 48 hours (7.78%), technical expertise (6.26%) or other patient-centred aspects of care. These findings, which represent patients' views, have important implications for service design.
INTRODUCTION
The evolution of sexual health clinics has largely been policy driven. The 48-hour waiting target 1 and the integration of contraception and sexually transmitted infection testing 2 have all led to major service changes. (It is hoped that by allocating more rapid access and a range of services under one roof the rates of sexually transmitted infections (STIs) 3 and unplanned pregnancy will be reduced. 4 )
However, little is known about what patients want from sexual health services. Published research has focused mainly on individual aspects of care such as confidentiality, 5 results management 6 and ‘one-stop shops’. 4 No assessment has been made of multiple domains of quality of care, for example organizational quality, interpersonal issues and technical quality (see the Methods section).
To address the issue of patient needs, we conducted a survey of patients attending an integrated sexual health service. We used a point allocation system 7,8 to determine what sexual health patients find most important about different aspects of sexual health care and whether this differs between those with primarily family planning or primarily genitourinary (GU) medicine needs.
The results of this survey can be used to direct resources in a more patient-oriented way.
METHODS
The survey took place in a walk-in integrated sexual health clinic in February 2009. The clinic is staffed by staff from the departments of GU medicine and sexual and reproductive health (formerly family planning) who are trained in both disciplines.
The clinic provides sexual health services to the residents of Enfield and its surrounding area, allowing patients to access both contraception and sexual health care in one setting. This ranges from an IUD or implant insertion to full STI testing and treatment (levels 1, 2 and 3 of the national sexual health strategy).
All patients attending the clinic were asked to complete an anonymous two-page questionnaire while waiting to be seen. The first page contained a brief introduction and asked them to ‘spend’ sticker coins by indicating with the coins the areas of sexual health that they found most important. A total of 10 stickers were provided and they could be distributed between 12 different attributes of sexual health care, each with an explanation (see Table 1). The order of questions was reversed after the first 100 forms were completed.
Sexual health care attributes
The issues were grouped into the following:
Impersonal care issues, e.g., choice of seeing a doctor or nurse and whether they are male or female, having issues explained fully, and seeing someone who is friendly and listens to them.
Organizational quality issues, e.g., rapid appointments, rapid test results, confidentiality and integrated services.
Technical quality issues, e.g., having expert medical care.
The second page asked about reason for attendance and demographic information.
The questionnaire was first piloted (SH) to ensure that patients filled in the form correctly and then validated by face-to-face interviews with patients (JA). During the validation process, patients were asked, after completing the questionnaire, about their understanding of the meaning of each sexual health issue (see Table 1). The 20 interviewees participating in the validation process agreed that the questionnaire was clear and easily understood.
Data from the completed questionnaires of the full study were entered into an Excel database. Ten percent of the questionnaires were double entered to ensure that there were no transcription errors. Simple descriptive analysis and χ2 testing were used where appropriate. The importance of an aspect of sexual health care was determined by calculating the number of stickers given to a particular health attribute as a proportion of the total number of stickers allocated by all participants and represented as a percentage.
The local research ethics committee was consulted regarding ethical approval. This was deemed unnecessary as the project was considered a service survey.
RESULTS
Two hundred and sixty-four questionnaires were handed out and 252 (95.45%) were returned.
All respondents completed page 1 of the questionnaire, which asked them about the value of various sexual health attributes, but 72 (28.57%) did not fully complete the demographic data section on page 2. In all, 180 (71.42%) completed the whole questionnaire.
Of the 180 (71.42%) who completed the whole questionnaire, 43 (23.88%) of the respondents were men and 137 (76.11%) were women. This was similar to the usual gender mix of those attending the integrated clinic where 72.44% are women and 27.55% are men. Likewise, the age and ethnicity distribution did not differ from that generally attending our integrated clinics.
This was the first attendance at a sexual health clinic for 87 (48.3%) respondents, with 90 (50%) attending primarily for contraception and 81 (45%) for sexually transmitted infection testing. Nine (5%) did not indicate either reason on their response form.
The total number of stickers allocated to all attributes was 2236 (of 2520 possible). One hundred and eighty-seven (74.2%) participants used all 10 stickers when completing the form and 12 (5.95%) used less than five stickers.
The most important sexual health attribute recorded by patients when attending a clinic was confidentiality (18.47% of all stickers allocated), followed by speed of service (13.1%) and rapid test results (12.12%). Being seen within 48 hours was less important (7.78). Attributes recorded as least important were receiving targeted care (2.91%) and having an alcohol, drugs and violence assessment (2.77%) (see Figure 1).
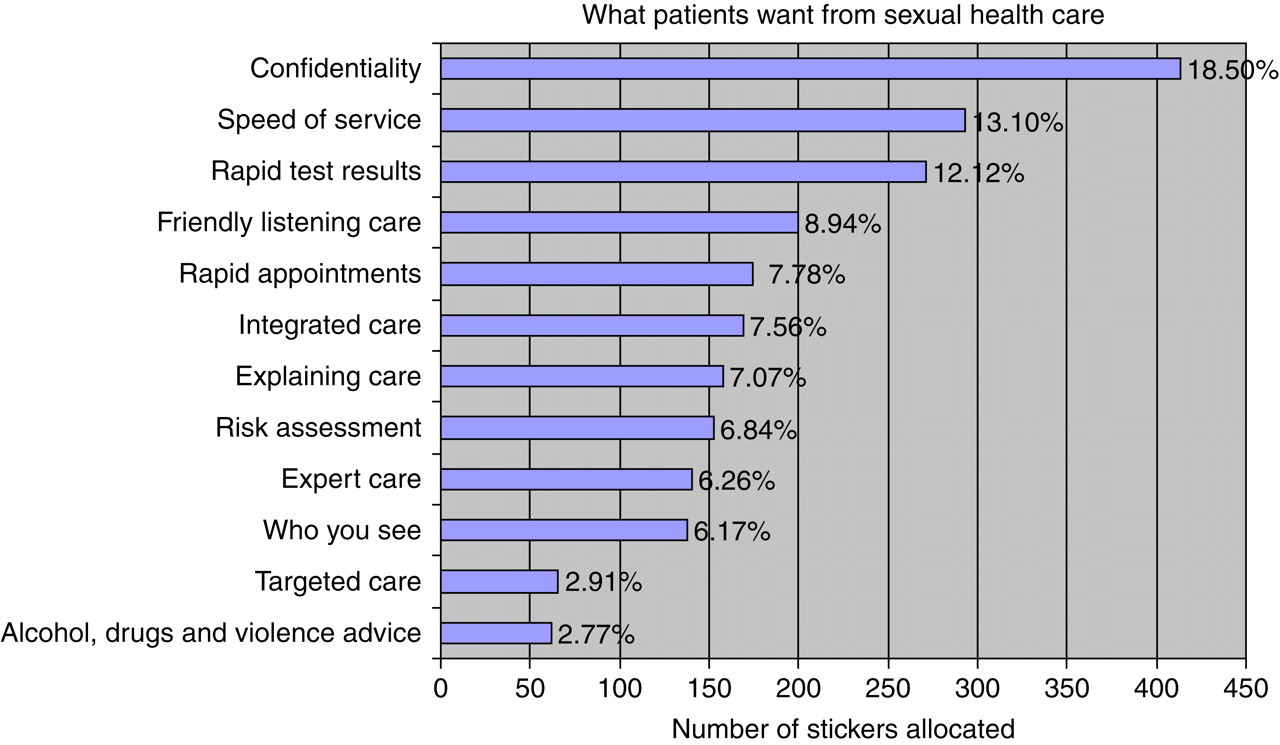
‘What patients want?’ Allocation of stickers to different sexual health-care attributes
Although overall nearly a fifth of the total stickers were given to confidentiality (413/2236), 20% (51/252) of individuals questioned gave confidentiality no stickers. A minority of respondents, 23% (60/252), effectively classed it as very important by giving it three or more of the 10 stickers.
When comparing those patients attending primarily for contraception, 20.3% ‘voted’ for confidentiality whereas 16.7% STI patients recorded this as being important (P = NS).
The allocation of stickers according to reason for attendance is set out in Table 2. Analysis of sticker allocation was grouped into 0 stickers (not important), 1 sticker (important) and 2 or more stickers (very important).
How respondents classed sexual health-care attributes according to reason for attendance
*Represents significance at the P < 0.05 level
STI = sexually transmitted infection
Table 2 shows that for most sexual health-care attributes, patients attending primarily for contraception had similar needs to those attending mainly for STI testing. However, those who attended mainly for STI tests were significantly more likely to value rapid test results (P = 0.0056, χ2 ).
There were no significant (P < 0.05) differences in sticker allocations observed between male and female respondents or young people aged 17 years and under compared with those aged 18 years and over.
DISCUSSION
To our knowledge, this is the first time sexual health-care patients have been asked to prioritize attributes of sexual health care that are given in a specialized clinic. The results are relevant as they reflect views of the patient. The validation undertaken on a purposive sample suggests that participants understood and liked the method devised for this purpose.
Our method of determining service user priorities was similar to points allocation, 6,7 but is not frequently used in health care. The pilot study showed that patients understood this novel method of questioning and that they found it more enjoyable than traditional questionnaires. We used it because we wanted to capture information on ‘spending’ limited resources. We therefore provided a finite number of stickers, so that it was not possible to class all aspects of care as being very important.
‘Willingness to pay’ could not be used as our patients came from a very diverse sociodemographic background, and hence the value of money differs between them. Furthermore, it would be a very artificial concept to pay for a free service.
We also felt that the discrete choice method, where patients had to decide between different scenarios, would be too time consuming for our patients. We discarded the use of 5-point Likert scales because we felt that many patients would give high values to many attributes, which would make it difficult to decide how to use scarce resources.
Ranking of attributes would have been possible, but is likely to have been more time consuming for the service user than points allocation. It might also encourage patients to give importance to areas they did not value just because they felt obliged to place all aspects in a list. 9
The high throughput of the service and the short waiting periods demanded a simple design of the form, which could be rapidly completed by our patients. We believe that the short waiting time partly explained why many patients did not complete the demographic second page of the questionnaire. Most of the participants completed the sticker allocation as directed.
From the 71% respondents who completed the whole questionnaire, we found that there was little difference in patient priorities between any of the demographic subgroups. Likewise, patients attending for contraception or STI-related care appeared to have similar priorities. This supports the integration of the two services that has occurred.
We have commented on the major findings below:
Confidentiality was the most important attribute. Despite this nearly a quarter of patients gave it no stickers and over half of the participants gave it one or no stickers, indicating that for them it was not the most important aspect of care. This group of patients may value other aspects of sexual health care above confidentiality or they may not be concerned about other health-care professionals having information on their sexual health care; Patients allocated most stickers to organizational aspects of care (speed of service, rapid results, confidentiality) and far less to technical aspects such as expert care. This may reflect their perception on the quality of care provided by the clinic. Similar prioritization may not be found in other clinics, especially if doubts exist about the quality of care. This is relevant when compared with the finding from surveys in the primary care sector, where medical expertise is often valued most highly;
10
UK government policy stresses the importance of rapid access to care (the 48-hour waiting time target) as well as the integration of sexual and reproductive health services. Our survey showed that rapid access did not have a high priority for our patients. What was given greater importance was receiving rapid test results and being seen quickly while in the clinic; The lowest scoring attribute was alcohol, drugs and violence assessment. As service users do not attend sexual health services specifically for these problems, the low rating of this attribute supports the validity of our assessment tool; We found that family planning patients were significantly less likely to value rapid test results. As most of them did not expect any tests, this finding supports the internal validity of our method. However, further research is required on the validity of the tool.
Our survey suggests that to meet the wishes of service users, sexual health services have to focus on confidentiality and the speed of service delivery. This appears more important than medical expertise, rapid access or patient centredness.
CONCLUSION
Points allocation is a feasible method to assess patient priorities in sexual health services. While the validity of the tool needs to be confirmed, our results indicate that patients value confidentiality (as expected) and rapid throughput and rapid test results more than any other attribute of care (such as technical expertise, waiting times and patient centredness). This has obvious implications for service design.