
Abstract
In a retrospective database study at two HIV treatment centres, medical records were accessed to evaluate long-term efficacy and safety parameters in all HIV-infected adults who had achieved HIV-1 RNA <50 copies/mL following the initiation of fosamprenavir (FPV)/ritonavir (RTV) 1400 mg/100 mg once-daily (QD)-containing regimens between January 2004 and January 2006. Data were available for 20 antiretroviral (ARV)-naïve patients (baseline median HIV-1 RNA 5.0 log10 copies/mL; CD4+ cell count 307 cells/mm3), 30 protease inhibitor (PI)-naïve, ARV-experienced patients (HIV-1 RNA 3.6 log10 copies/mL; CD4+ count 348 cells/mm3) and 25 PI-experienced patients switching to FPV/RTV100 for reasons other than virological failure (HIV-1 RNA 2.7 log10 copies/mL; CD4+ count 328 cells/mm3). HIV-1 RNA <50 copies/mL was achieved in 100% of the ARV-naïve cohort (median monitoring period, 2.4 years; range, 1.4–3.2 years), 87% of the PI-naïve cohort (2.4 years; range, 1.2–3.4 years) and 88% of the PI-experienced cohort (2.2 years; range, 1.0–3.2 years). Virological failure occurred in 0%, 7% and 8% of the cohorts, respectively, and median CD4+ count increased above baseline by 224, 155 and 115 cells/mm3, respectively. Change from baseline in median fasting lipids was: total cholesterol +12, −6, −2 mg/dL; low-density lipoprotein-cholesterol 0, −5, +12 mg/dL; high-density lipoprotein-cholesterol +4, +2, +7 mg/dL; triglycerides +9, −21, −65 mg/dL, respectively. In conclusion, FPV/RTV 1400/100 mg QD-containing regimens remained effective long-term in all ARV-naïve and most PI-naïve and PI-experienced HIV-infected patients.
INTRODUCTION
In SOLO, once-daily (QD) fosamprenavir (FPV) 1400 mg boosted by ritonavir (RTV) 200 mg QD, plus twice-daily abacavir/lamivudine (ABC/3TC) 300 mg/150 mg, allowed 69% of 322 antiretroviral (ARV)-naïve, HIV-infected patients to achieve viral loads (VL) <400 copies/mL by 48 weeks. 1 Subsequently, a lower RTV boosting dose of 100 mg QD, co-administered with FPV 1400 mg QD, was found to provide minimum concentrations of FPV's active metabolite, APV, six-fold higher than the protein binding-corrected 50% inhibitory concentration (IC50) for wild-type HIV (0.146 µg/mL) 2 and to produce virological suppression similar to RTV 200-mg boosted FPV regimens, with generally less lipid elevation. 3–7 However, most of these studies were of short duration and included only ARV-naïve patients. The purpose of the present study, BOLD100, was to evaluate the long-term efficacy/safety of FPV/RTV 1400/100 mg QD-based regimens in three cohorts: ARV-naïve patients and protease inhibitor (PI)-naïve and PI-experienced patients who switched to FPV/RTV for reasons other than virological failure.
MATERIALS AND METHODS
This retrospective database study was conducted at two HIV treatment centres (CIRCLE Medical LLC in Norwalk, CT, USA and Mt Vernon Hospital in Mt Vernon, NY, USA) to investigate treatment response of HIV-seropositive patients who started an ARV regimen containing FPV/RTV 1400/100 mg QD (FPV/RTV100) between January 2004 and January 2006 and continued it for at least six months. Data could be included in this study only for patients with an HIV-1 RNA level ≥1000 copies/mL, any CD4+ cell count and no active AIDS-related infections/complications/malignancies. The medical records of qualifying patients were manually checked by study personnel who captured data on Excel spreadsheets pertaining to demographics, HIV history, duration of FPV/RTV100 usage, background ARV therapy, non-ARV medication usage, discontinuation/change in regimens, HIV-1 RNA changes (proportion <50 and <400 copies/mL), occurrence/time of virological failure (defined as decrease in HIV-1 RNA to <400 copies/mL with subsequent increase to ≥400 copies/mL on two consecutive occasions or failure to achieve <400 copies/mL by week 24), CD4+ cell count changes and adverse clinical/laboratory events. Statistics were descriptive in the observed population.
RESULTS
Data were available for 20 previously ARV-naïve patients, 30 PI-naive patients and 25 PI-experienced patients who switched to FPV/RTV100-containing regimens for reasons other than virological failure (Table 1). The cohorts were diverse with respect to race and gender. In the ARV-naïve cohort, which was monitored over a median of 2.4 years (range, 1.4–3.2 years), all patients achieved HIV-1 RNA <50 copies/mL, no virological failures occurred and CD4+ cell counts increased steadily (Figure 1), with a median +224 cell/mm3 change from baseline (BL) by the end of the monitoring period. In all three cohorts, several patients withdrew from the study over the course of therapy, especially after two years, for reasons not related to adverse events or efficacy issues (i.e. loss to follow-up, protocol violation, non-compliance or patient's decision to withdraw). Adverse events were generally grades 1 and 2, and included diarrhoea, nausea and vomiting (Table 2). Increases in fasting total cholesterol, high-density lipoprotein (HDL)-cholesterol and triglycerides were observed; in the case of triglycerides, the median rose 2 mg/dL above the National Cholesterol Education Programme (NCEP) cut-off level 8 (Figure 2).
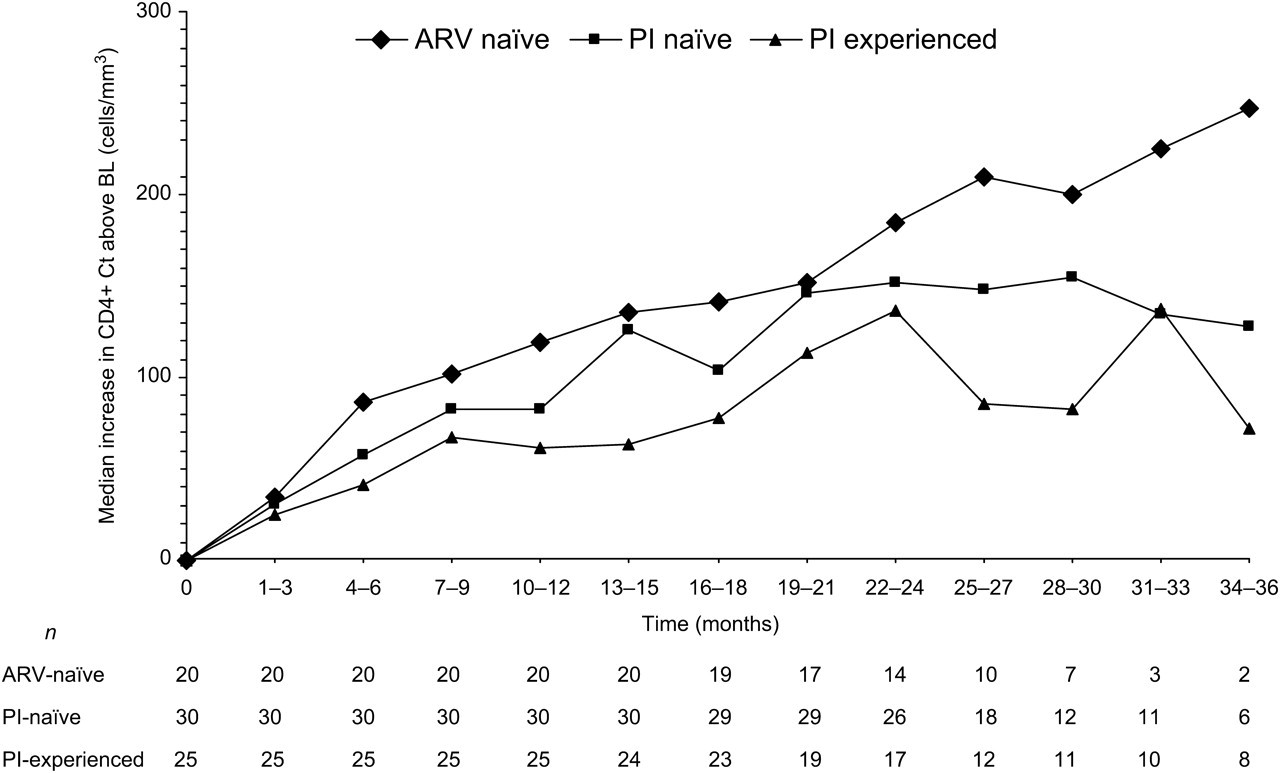
CD4+ count change from baseline (BL). ARV = antiretroviral; PI = protease inhibitor

Change from baseline in median fasting lipids of 75 patients taking FPV/RTV100. NCEP c/o = National Cholesterol Education Programme cut-off level; Tot = total; HDL = high-density lipoprotein; LDL = low-density lipoprotein; TGs = triglycerides
Demographics and BL characteristics of ARV-naïve (n = 20) and -experienced patients (n = 55)
BL = baseline; MSM = men who have sex with men; Het = heterosexual; IDU = injecting drug user; HCV = hepatitis C virus; HBV = hepatitis B virus; PCR = polymerase chain reaction; ABC = abacavir; ARV = antiretroviral; ddI = didanosine; EFV = efavirenz; FTC = emtricitabine; FPV = fosamprenavir; NRTI = nucleoside reverse transcriptase inhibitor; NNRTI = non-nucleoside reverse transcriptase inhibitor; PI = protease inhibitor; RTV = ritonavir; 3TC = lamivudine; TDF = tenofovir disoproxil fumarate; ZDV = zidovudine
*Four-drug combinations were most commonly ABC/ZDV/3TC/TDF, ABC/ddI/FTC/TDF and ddI/EFV/FTC/TDF
Efficacy and safety results of 75 patients taking FPV/RTV100
ARV = antiretroviral; BL = baseline; Δ from BL = change from baseline; FPV = fosamprenavir; HDL = high-density lipoprotein; LDL = low-density lipoprotein; RTV = ritonavir; MRSA = methicillin-resistant Staphylococcus aureus; PI = protease inhibitor
*Defined as viral load decrease to <400 copies/mL, followed by increase to ≥400 copies/mL on two consecutive occasions, or not achieving <400 copies/mL by week 48 following treatment initiation
†Grade 1
In the PI-naïve cohort, the median monitoring period was 2.4 years (range, 1.2–3.4 years). Reasons for switching to FPV/RTV100 were viral rebound (23), efavirenz intolerance (3), peripheral neuropathy (1), zidovudine intolerance (1), pancreatitis (1) or need for regimen simplification (1). ARV medications discontinued following the switch to FPV/RTV100-containing regimens included efavirenz, nevirapine, zidovudine, ABC, didanosine, 3TC, stavudine, tenofovir and emtricitabine.
In the PI-experienced cohort, the median monitoring period was 2.2 years (range, 1.0–3.2 years). The most common reasons for switching to FPV/RTV100 were lopinavir intolerance (diarrhoea, hypertriglyceridaemia, hypercholesterolaemia) (7), need for regimen simplification (4), atazanavir intolerance (hyperbilirubinaemia, drug interactions with proton pump inhibitors) (8), viral rebound (2), need for intensification (1) and intolerance to tipranavir (1), amprenavir (1) or efavirenz (1). Following the switch to FPV/RTV100 by the PI-naïve and PI-experienced cohorts, virological failure occurred in 7% and 8%, respectively. At the last study visit, HIV-1 RNA <50 copies/mL was achieved in 87% and 88% and median CD4+ cell count increased above baseline by 155 and 115 cells/mm3 in the PI-naïve and PI-experienced cohorts, respectively. Small changes in fasting total, low-density lipoprotein (LDL)- and HDL-cholesterol were observed, whereas triglycerides decreased modestly (−21 and −65 mg/dL, respectively) after the switch to FPV/RTV100 (Table 2).
DISCUSSION
The long-term efficacy findings of this retrospective patient chart review study support the results of shorter-term clinical trials that have evaluated FPV/RTV100 mg QD-containing regimens in ARV-naïve patients over 24–48 weeks. 4–7 Thus, DeWit et al. 6 found at 48 weeks that 86% of 54 ARV-naïve patients (median BL VL 4.9 log10 copies/mL, CD4+ count 171 cells/mm3) treated with FPV/RTV100 plus either a TDF/3TC or TDF/FTC backbone QD achieved a VL <50 copies/mL and a median CD4+ cell increase above BL of 268 cells/mm3 (intent to treat: observed analysis). Similarly, in ALERT, 89% of 53 ARV-naïve patients (median BL VL 4.9 log10 copies/mL, CD4+ count 161 cells/mm3) treated with FPV/RTV100+ ABC/3TC QD had a VL <50 copies/mL at 48 weeks (intent to treat: observed analysis). 4 The fact that the efficacy rate of our ARV-naïve cohort was even higher than that in the above trials may have been due largely to our patients’ better immunological status at BL, with the median BL CD4+ count being about twice that (307 cells/mm3) of patients in the DeWit et al. 6 and ALERT 4 studies. More recently, the 96-week results of COL100758 were presented, which corroborated long-term virological suppression with FPV/RTV100 + ABC/3TC QD and indicated a trend for a larger proportion of patients achieving a VL <50 copies/mL with this regimen than with twice the RTV dose (200 mg QD) (66% [38/58] versus 53% [30/57]) regardless of BL VL strata (<100,000 versus ≥100,000 copies/mL). 9 It is worth noting however, COL100758 was not designed to be a fully powered study, and the higher VL (median, 4.9 versus 4.7 log10 copies/mL) and lower CD4+ count (median, 259 versus 179 cells/mm3) in the RTV 200 mg QD arm at baseline may possibly have impacted the study outcome.
The safety profile we observed for FPV/RTV100-containing regimens is consistent with that reported for these regimens in other clinical trials. 3–7,9 Grades 1 and 2 diarrhoea, nausea and vomiting are the most frequently reported adverse events, and the occurrence and severity of these tend to lessen over time. This is especially noticeable when one compares the gastrointestinal adverse event frequency of our ARV-naïve cohort with that of our PI-naïve and PI-experienced patient cohorts. Although our study did not compare the frequency of adverse events in FPV/RTV100-treated patients with that in FPV/RTV200-treated patients, where such comparisons have been done, the incidence of gastrointestinal adverse events has been reported to be either lower or not notably different with FPV/RTV100 regimens. 3,7,9 The small increases in fasting total, LDL- and HDL-cholesterol and modest increase in triglycerides observed in our ARV-naïve cohort has been observed in other clinical trials. 4,6,7,9 In these, the elevation in triglycerides has generally been the only lipid parameter that exceeds, to a varying degree, the NCEP cut off. 8 In studies that have compared fasting lipids between FPV/RTV100- and FPV/RTV200-containing regimens, FPV/RTV100 was generally associated with either slightly lower or similar total-, LDL- and HDL-cholesterol levels, but modestly lower triglycerides. 3,7
This retrospective study is the first to gather data in a formal manner on FPV/RTV100-containing regimens in ARV-experienced patients. An indication for using such regimens in this population is currently not approved in any country because of concern that patients harbouring resistance to PIs may not respond adequately. Ruane et al. 3 found that the mean APV trough concentration following FPV/RTV100 was 0.86 µg/mL, which is slightly lower than the mean APV protein binding-adjusted IC50 value for multiple PI-resistant HIV (0.90 µg/mL). 10 It is therefore reassuring that >85% of our PI-naïve and PI-experienced patients achieved a VL <50 copies/mL after switching to FPV/RTV100, and that their CD4+ cell count continued to increase over the entire monitoring period. This suggests little likelihood that these patients had resistance to APV.
The modest decrease in triglycerides and smaller decreases in total and LDL-cholesterol that were observed in the PI-naïve and PI-experienced cohorts were likely due mainly to the lower RTV boosting dose to which these patients were switched. RTV-associated lipid elevations have been well documented as dose related. 11 Reduction in the RTV boosting dose from 200 mg QD to 100 mg QD by itself has been reported to prompt reduction in triglycerides within four weeks. 12–14 The fall in triglycerides may also have been secondary to discontinuation of previous agents, such as efavirenz, nevirapine, stavudine, didanosine, lopinavir and tipranavir, which have been reported to increase lipids. 15–19
This study of patient medical records was limited by the small population studied and by its retrospective design. Several patients withdrew from the study for reasons unrelated to efficacy or safety, and this limited the evaluation of response beyond the two-year time point. No data were available about the patients’ dietary or lifestyle changes, or resistance test results during therapy.
CONCLUSIONS
In this retrospective trial, FPV/RTV100-containing regimens remained effective long-term in all ARV-naïve and most PI-naïve and PI-experienced HIV-infected patients.