
Abstract
The aim of the present study is to investigate the rate of co-infections with other sexually transmitted infections (STIs), antibiotic susceptibility and management of oropharyngeal gonorrhoea diagnosed in a busy genitourinary medicine clinic. The method involved a retrospective study on consecutive patients diagnosed with oropharyngeal gonorrhoea. A total of 131 patients were diagnosed with oropharyngeal gonorrhoea over the study period. The median age of the infected patients was 28 (interquartile range: 22 to 35) years. Forty-one (31%) of patients were younger than 24 years. High rates of co-infection with urethral gonorrhoea (37%), rectal gonorrhoea (37%) or chlamydial infection (16%) were identified. Thirty patients (23%) had only oropharyngeal infection. Twenty-two (17%) patients' isolates showed resistance to at least one antibiotic. Antibiotic resistance among oropharyngeal gonococcal isolates was above 5% between 2000 and 2009. Test-of-cure (TOC) was carried out for only 63 (48%) of patients; none had positive culture. Among 46 isolates treated with cefixime 400 mg/stat, 27 (59%) had TOC; all were negative. Repeat TOC was not carried out for any of the patients. In conclusion, successful management of oropharyngeal gonorrhoea should comprise of counselling, partner notification and TOC after treatment with appropriate antibiotic regimen.
BACKGROUND
Between 2000 and 2007, more than 18,000 of new cases of gonococcal infection have been diagnosed in the UK each year. 1 A significant proportion of those patients have been diagnosed with oropharyngeal gonorrhoea.
Oropharyngeal gonorrhoea rarely causes symptoms and has been shown to be difficult to detect most likely due to insensitive sampling techniques. 2,3 In the UK, screening for oropharyngeal gonorrhoea is recommended when indicated by sexual history. 4
The aim of the present study was to investigate the rate of co-infections with other sexually transmitted infections (STIs), antibiotic susceptibility and management of oropharyngeal gonorrhoea diagnosed in a busy genitourinary medicine clinic.
METHODS
This was a retrospective study on consecutive patients diagnosed with oropharyngeal gonorrhoea at the Department of Genitourinary Medicine at Whittall Street Clinic between 1 January 2001 and 1 January 2008.
Oropharyngeal gonorrhoea was diagnosed by inoculation at bedside of the material obtained from the oropharynx and tonsils over Modified New York City Culture Medium (MNYC). According to the department's policy, patients with oropharyngeal gonorrhoea were asked to return to the clinic for test-of-cure (TOC) seven days after treatment. An appointment for repeat TOC 14 days after treatment was also arranged.
Screening for C. trachomatis was carried out by testing urine specimens with the BD ProbeTecET© strand displacement amplification assay (Becton-Dickinson Diagnostic Systems, Sparks, MD) according to the manufacturer's instructions. Serology specimens were tested for HIV and syphilis according to the national guidelines.
The list of patients with culture-positive pharyngeal gonorrhoea during the above period was provided by the microbiology laboratory at University Hospitals Birmingham.
Case-notes of patients were reviewed and notes were taken on their age, ethnic background, antibiotic susceptibility profile of each isolate, antibiotic regimen and the result of TOC. Results of screening for chlamydia, syphilis and HIV were also recorded.
Susceptibility profile was determined for penicillin, tetracycline, ciprofloxacin, spectinomycin, azithromycin and ceftriaxone and reported as minimum inhibitory concentration (MIC).
Data were recorded on a spreadsheet. The median values with interquartile range (IQR) for non-parametric data were calculated.
RESULTS
A total of 131 patients were diagnosed with oropharyngeal gonorrhoea over the study period. This included 83 (63%) men who have sex with men (MSM), and 100 (76%) patients of white ethnicity. The median age of the infected patients was 28 (IQR: 22 to 35) years. Forty-one (31%) of patients were younger than 24 years. Presence of oropharyngeal symptoms was enquired about from 68 (52%) of patients; four (5%) reported sore throat.
Patients with oropharyngeal gonorrhoea had a high rate of gonococcal infection of anogenital sites, chlamydial and HIV infections (Table 1). Thirty patients (23%) had only oropharyngeal infection.
The rate of co-infection with sexually transmitted infections amongst patients with oropharyngeal gonorrhoea
HBcAb: Hepatitis B core antibody
HBsAg: Hepatitis B surface antigen
*Urethral chlamydia in men and cervical chlamydia in women
Antibiotic susceptibility assays were available for 128 (98%) patients; 22 (17%) of whom had resistance to at least one antibiotic. Table 2 summarizes the prevalence of resistance to different antibiotics. The incidence of antibiotic-resistant gonococcal isolates during the study period is summarized in Figure 1. It shows antibiotic resistance among oropharyngeal gonococci isolates was above 5% between 2000 and 2009.
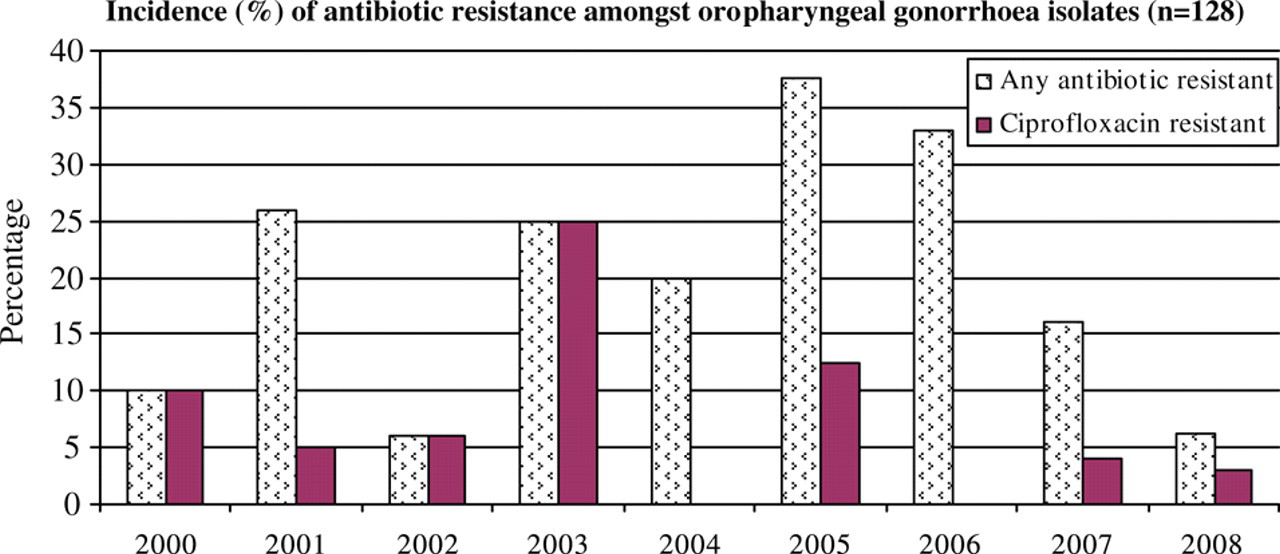
Incidence (%) of antibiotic resistance among oro-pharyngeal gonorrhoea isolates (n = 128)
Antibiotic susceptibility of 128 oropharyngeal isolates of gonorrhoea
TOC was carried out for only 63 (48%) of patients; none of whom had positive culture. Repeat TOC was not carried out for any of the patients.
Amongst the 131 patients with oropharyngeal gonorrhoea, 128 (98%) were treated. Four isolates resistant to ciprofloxacin were treated with ciprofloxacin 500 mg/stat and doxycycline 100 mg/bd for seven days; three patients had negative gonorrhoea culture seven days after completion of treatment.
Amongst 46 isolates treated with cefixime 400 mg/stat, 27 (59%) had TOC; all were negative.
DISCUSSION
Oropharyngeal gonorrhoea remains an elusive infection that contributes to the spread of gonococcal infection. 5,6 Very few infected patients report symptoms and these are non-specific and may be easily ignored.
The majority of patients in the present study were of white ethnicity, MSM, younger than 24 years of age and had co-infection with another STI. Because of its association with oral sex, oropharyngeal gonorrhoea might not be considered as a marker of high risk sexual behaviour. Our data, however, suggest otherwise; a high rate of chlamydial, HIV, hepatitis B and ano-genital gonococcal infections were diagnosed amongst patients with oropharyngeal gonorrhoea.
The rate of resistance to penicillin and ciprofloxacin in oropharyngeal isolates was alarming. The rate of ciprofloxacin-resistant Neisseria gonorhoeae isolated from oropharyngeal specimens reached 25% in 2003 and has fallen since. The overall rate of ciprofloxacin-resistant N. gonorrhoeae in the UK has been increasing since 2003, reaching 27% in 2007. 7 It is important to treat oropharyngeal gonorrhoea with an effective antibiotic; none of the patients were resistant to cefixime. Use of cefixime for treatment of oropharyngeal gonorrhoea was associated with 100% success rate in the present study. Similar treatment outcome with cefixime has been reported previously. 8 It is important to note that treatment failure of oropharyngeal gonorrhoea with cefixime has also been reported. 9
Treatment of oropharyngeal gonorrhoea may fail in a proportion of patients. 8–11 Treatment failure amongst a significant proportion of oropharyngeal N. gonorrhoeae isolates may occur despite having been treated with an antibiotic to which they were susceptible. 11 Treatment failure was not documented in any patients with TOC. Conduct of TOC therefore remains an important part of the management of oropharyngeal gonorrhoea.
In the present study TOC was not carried out in a significant proportion of patients. Patients' failure to attend the department for TOC was the most common reason for this. Treatment failure was not documented in any of patients with TOC. Screening for HIV and syphilis was not carried out in a significant proportion of patients who declined the tests. Twenty-six of the 82 MSM also declined screening for rectal gonorrhoea.
In the present study showed that oropharyngeal gonorrhoea could be associated with high-risk sexual activity as indicated by the high rates of co-infection with anogenital STIs. Antibiotic-resistant strains accounted for a significant proportion of cases of oropharyngeal gonorrhoea. This highlights the need for counselling, partner notification and TOC after treatment of oropharyngeal gonorrhoea with appropriate antibiotic.