
Abstract
We describe a 77-year-old patient with HIV infection suffering from chronic diarrhoea whose colonoscopy findings showed normal appearance mucosa and tissue samples revealed the presence of a dense layer of spirochetes attached to the apical cell membrane. A literature search from 1996 to April 2009 identified 19 additional cases of intestinal spirochetosis in patients with HIV infection. Analysis of cases showed that intestinal spirochetosis causes chronic diarrhoea in men who have sex with men (92% of patients with reported HIV infection risk factors) who are not severely immunosuppressed (70% with CD4 lymphocyte cells >200/μL). Colonoscopy examination often revealed normal appearance mucosa. Haematoxylin and eosin stain of biopsy samples showed the presence of spirochetes, but Warthin–Starry silver staining makes organisms easier to detect. Patients promptly responded to metronidazole or penicillin therapy. In summary, invasive intestinal spirochetosis should be considered in the differential diagnosis of patients with HIV infection and chronic diarrhoea.
INTRODUCTION
Despite the introduction of combination active antiretroviral therapy, 40% of HIV-infected adults still suffered one episode of diarrhoea in the preceding month in a study carried out in the Boston area. Chronic diarrhoea (defined as ≥28 days of diarrhoea) was reported in 28% of this cohort and severe diarrhoea (defined as more than 6 stools per day) in 3%. 1 Diarrhoeal disease in HIV-infected patients can be due to a multitude of aetiologies from infectious pathogens to malignancy to medications. Herein we report an unusual case of chronic severe diarrhoea caused by colonic invasion of spirochetal microorganisms in an elderly patient with HIV infection and review the literature on intestinal spirochetosis in the era of combination antiretroviral therapy.
CASE REPORT
A 77-year-old man with an eight-year history of HIV infection attended our HIV clinic suffering from chronic diarrhoea. He suffered from five loose stools per day without blood, abdominal pain, vomiting or fever in the last two months. His adherence to antiretroviral therapy was good and his current regimen with ritonavir-boosted lopinavir, tenofovir and stavudine started coincidentally with the patient's diarrhoea. His last CD4 lymphocyte cell count was 529 cells/μL and the HIV-1 RNA was 1200 copies/mL. Physical examination revealed diffuse abdominal tenderness. Vital signs were normal. Stool studies were negative. Patient's diarrhoea was initially attributed to lopinavir–ritonavir therapy and he received racecadotril as antidiarrhoeal drug without improvement. Colonoscopic examination did not show any gross abnormalities. However, colon biopsies showed the presence of a dense layer of spirochetes attached to the brush border of the colon mucosa and the presence of chronic non-specific inflammation in the lamina propria (Figure 1). The patient was treated with metronidazole 500 mg every eight hours for three weeks with resolution of symptoms. Repeated colonoscopy and colon biopsies revealed organism eradication.
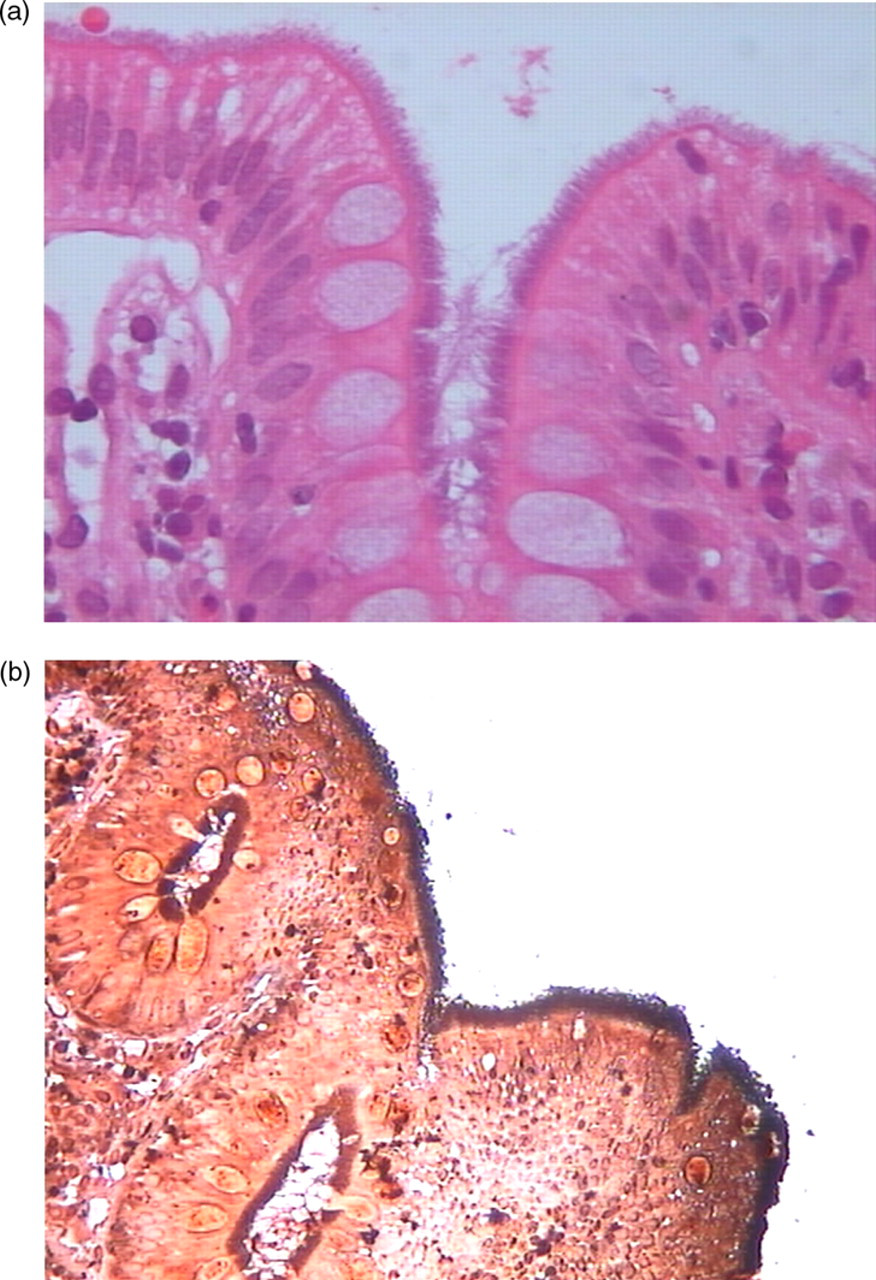
(a) Haematoxylin–eosin stain shows a fuzzy coat of spirochetes attached to the surface of the colonic mucosa (light microscopy × 400). (b) Warthin–Starry silver stain highlights the organisms as a darkly stained black border (light microscopy × 200)
DISCUSSION
Intestinal spirochetosis caused by bacteria from genus Brachyspira has been isolated from pigs, chickens, dogs and humans. Based on genomic DNA sequence analysis, the two members of Brachyspiraceae family most commonly associated with the human disease are Brachyspira aalborgi and Brachyspira pilosicoli. Cases of chronic diarrhoea caused by invasive infections have been reported in non-immunosuppressed patients from developing countries, homosexual men and patients with HIV infection 2 (Table 1).
Summary of data on invasive intestinal spirochetosis in patients with HIV infection
MSM = men who have sex with men; NR = not reported; PR = present report; PCR = polymerase chain reaction
We carried out a literature search in MEDLINE electronic database from 1996 to April 2009 using (Brachyspira OR Spirochetosis OR Serpulina) AND Diarrhoea AND HIV as a search strategy. In addition, we scanned the reference list from the identified articles.
A total of 20 cases (including the present report) were analysed. 3–15 All reported cases were HIV-infected male patients from developed countries, 83% with known HIV transmission category were men who have sex with men (MSM). Seven out of 10 patients with available CD4 lymphocyte counts had >200 cells/μL. Colonoscopy often showed a normal mucosa, mild erythema or polypoid areas. Colon biopsies showed the presence of spirochetes oriented perpendicular to the mucosal surface with destruction of microvilli and mild inflammatory infiltrate in the lamina propria. Warthin–Starry silver staining of tissue allowed a better visualization of spirochetes than haematoxylin–eosin stain. Identification of up to species level by means of polymerase chain reaction amplification in faecal or fixed tissue samples showed B. aalborgy in seven cases, B. pilosicoli in three cases and both B. aalborgy and B. pilosicoli in one case. Therapy with metronidazole or penicillin led to the resolution of symptoms in every case.
The prevalence of intestinal spirochetosis is reported to be 2–7% in Western countries, 11–34% in less developed countries and up to 54% in MSM and HIV-infected patients. 16 Although chronic diarrhoea was the most common presentation with mild inflammation or normal-appearing colon mucosa, some of the reported patients in the era previous to combination antiretroviral therapy suffered from severe acute inflammatory reactions with crypt abscesses and ulcers. 17 Spirochetes can cause bloodstream infections, but identification is often clinically missed since detection time in automated systems exceeded five days under anaerobic conditions. 18 Most patients with spirochetemia suffered from severe underlying disease and/or immunosuppression leading to death in more than two-thirds of cases; among the reported cases there was a male patient suffering from AIDS and Kaposi's sarcoma. Spirochetemia is likely originated in the intestinal tract by translocation or increased mucosal permeability since, in such cases, bloodstream isolates often closely related to faecal isolates.
In summary, clinicians should maintain a high index of suspicion of intestinal spirochetosis in HIV-infected patients suffering from chronic diarrhoea. MSM are more often affected than other HIV transmission categories.