
Abstract
Audit of gonorrhoea management resulted in recognition of a need to change the clinic protocol for first-line antibiotic therapy and also in improvements in clinic recording of written information given to patients and the outcome of contact tracing.
INTRODUCTION
Neisseria gonorrhoeae is a common sexually transmitted infection (STI) in the UK. National standards have been set for management. 1
This audit was undertaken in an urban genitourinary medicine clinic. The aim was to measure adherence to the five criteria stated in the national guideline published by the British Association for Sexual Health and HIV (BASHH). 1
METHODS
Local microbiology laboratory data and genitourinary medicine clinic health adviser (HA) records were used to perform a retrospective audit of all microbiologically confirmed cases of gonorrhoea who attended Coventry and Warwickshire Hospital Genito-Urinary Medicine clinic in the 12-month period from 1 October 2005 to 30 September 2006. Previous laboratory audit data had indicated low rates of penicillin resistance. Data from 147 cases from which one or more specimens resulted in positive cultures for N. gonorrhoeae were analysed. This included three positive rectal and six positive pharyngeal cultures. Mean patient age was 24.9 years (range 15–62 years). Further epidemiological characteristics are given in Figures 1 and 2. Patients were also offered other screening tests, including for chlamydia, using the BD ProbeTec strand displacement amplification assay (Becton, Dickinson & Company, Sparks, MD, USA).

Gender and sexual orientation of cases. MSM = men who have sex with men
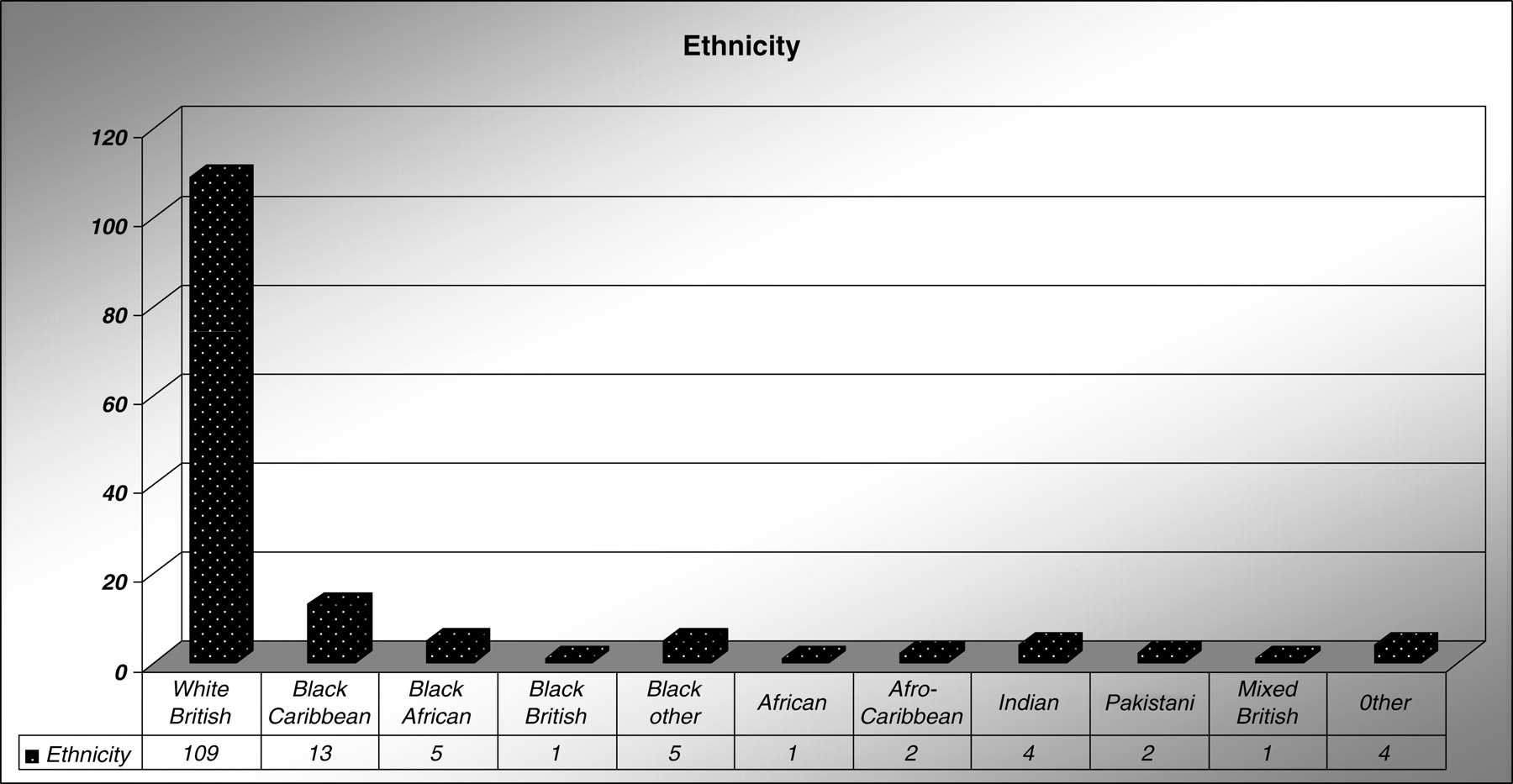
Ethnicity of cases, using standard Department of Health ethnicity criteria
RESULTS
I. ‘At least 95% of cases of genital gonorrhoea should be cured by first line therapy.’
1
At the time of the audit period, the usual first-line therapy was amoxicillin 3 g plus probenecid 1 g as a single dose. Of the 147 cases, 86/147 (58.5%) were treated with this. Twenty-three required re-treatment. Nineteen cases were because of antibiotic resistance and four because of either recent sexual history and/or recurrent symptoms presumed due to re-infection. Other first-line treatments that were used were cefixime 400 mg (n = 13), intramuscular ceftriaxone 250 mg (n = 9), ciprofloxacin 500 mg (n = 35) and azithromycin 1 g (n = 4). Of those treated by first-line therapy, 91/147 (61.9%) would have been cured if all had received penicillin. In fact, a variety of other first-line therapies were used, usually because of known reported antibiotic sensitivities as indicated in Table 1.
Gonorrhoea resistance patterns
Note: Two samples were not analysed for ciprofloxacin sensitivity
II. ‘All patients with gonorrhoea should be screened for genital infection with Chlamydia trachomatis or receive presumptive treatment for this infection.’
1
All 147 (100%) cases were screened for chlamydia and other STIs. Sixty-eight (46%) were co-infected with other STIs, 61 (41.5%) tested positive for chlamydia. Two had proven active genital herpes simplex. Five were diagnosed with genital warts. HIV test was offered to all, other than to the four who were known to be positive. In total, 90/143 (62.9%) accepted; all HIV tests performed were negative. III. ‘All patients identified with gonorrhoea should have at least one documented interview with a health adviser (HA) in GU Medicine or other health professional trained in partner notification and their action documented.’
1
Of the 147 cases, 136 (92.5%) saw an HA and contact tracing was discussed and documented. Four refused to see an HA and three were referred but left the department before being seen. Three were arranged subsequent HA appointments, but did not attend. One was not referred. No distinguishing epidemiological characteristics of the 11 who were not reviewed by an HA were observed. IV. ‘All patients identified with gonorrhoea should receive written information about sexually transmitted infections and their prevention.’
1
At the time of the audit, standard practice in the department was for all patients with gonorrhoea seen by HAs to be given written information. However, at the time of audit, specific documentation of provision of written information was not usually recorded. It was not possible therefore to accurately assess practice against this standard. V. ‘For all cases of gonorrhoea, at least 0.6 sexual partners should be verified as having been satisfactorily managed within 4 weeks. This rate of management of sexual partners may be unachievable in departments in some large cities and a lower rate may need to be locally determined.’
1
One hundred and forty-seven patients disclosed a total of 244 sexual partners during the three months prior to diagnosis. Of those partners, 148 were reported as contactable. Fifty-two recent sexual partners were confirmed as being treated by HAs. For every case, 0.35 sexual partners were verified as having been treated.
DISCUSSION
Only one of five BASHH audit criteria was fulfilled. Rates of penicillin and ciprofloxacin resistance in the current audit were similar to those reported as the regional rate for West Midlands for 2006. 2 In contrast, Coventry GU Medicine Clinic resistance rates prior to 2005 were reported to have been significantly lower than the equivalent regional rates. A previous audit of 115 cases in 2002 had demonstrated that 95.7% of gonorrhoea isolates were penicillin-sensitive, but only 86.1% were ciprofloxacin-sensitive: hence the reason for amoxicillin and probenecid remaining as the first-line treatment at the time of commencing the recent audit. The reasons for this local increase in antibiotic resistance are unclear. It is noted that BASHH Guidelines 1 do not recommend azithromycin for gonorrhoea. Concerns have been raised as to whether pharyngeal gonorrhoea is reliably treated by oral cefixime. However, a report of an audit of the efficacy treatment of pharyngeal gonorrhoea with a single oral dose of 400 mg of cefixime has indicated high rates of cure with this therapy. 3
Based on regional and local data emerging, first-line therapy for the clinic was changed to either cefixime 400 mg stat orally or ceftriaxone 250 mg stat intramuscularly prior to completion of the audit. Documentation of contact tracing is undertaken by HAs. Contact tracing rates were similar to those reported in a previous similar audit. 4 However, it is thought that not all contacts treated were cross-referenced in HA records as having been treated. An improved electronic database system has now been introduced. The benefit of documentation of whether an information leaflet was given by HAs was recognized and clinic policy amended. A re-audit is planned. With improved documentation as described, an acceptable local rate of management of sexual partners may be determined as per BASHH guidelines.