
Abstract
Bacterial vaginosis (BV) is a common disorder of the genital tract in women characterized by an alteration of the normal acidic lactobacilli-predominant vaginal ecosystem to a vaginal environment dominated by Gardnerella vaginalis, mycoplasma species and anaerobes, with an increase in pH. The present study evaluated whether BV is associated with reproductive complications in women. BV was screened with a Gram stain of vaginal smear and interpretation was done using the Nugent score. Wet mount and polymerase chain reaction were used to screen other infections. Among 510 enrolled women, 72 (14.1%) had BV. Statistical analysis between the BV negative and positive population revealed a significant association (P = 0.0001) with infertility. In pregnant women, the infection rate was low (P = 0.01). Multiple infections such as Candida, Chlamydia and human papilloma virus were observed in 4.2%, 15.3% and 8.3% of BV-infected women, respectively. Results suggest that BV infection is associated with infertility and its absence leads to pregnancy, emphasizing its screening and treatment.
INTRODUCTION
The vagina has an environment with a multitude of microbiological species in variable quantities and relative proportions, which form a balanced ecosystem and provide defence against infection. In women, bacterial vaginosis (BV) is characterized by an alteration of the normal acidic lactobacilli-predominant vaginal ecosystem to a vaginal milieu dominated by organisms such as Gardnerella vaginilis, Mycoplasma sp. and anaerobes, with an accompanying increase in pH. 1 The most recent National Institute of Child Health and Human Development (NICHD) study on women at low risk for pregnancy complications was unable to show any effect of the presence of BV and its treatment on the rate of preterm birth, and preterm rupture of membranes and chorioamnionitis. 2 Previously, several groups had found that bacterial vaginal flora has an important impact on these complications. BV is considered the leading cause of vaginal discharge and malodour, 3 associated with adverse pregnancy outcomes, 4 pelvic inflammatory disease, 5 postoperative pelvic infections 6 and a higher prevalence of HIV among certain high-risk populations. 7,8 However, there is a paucity of information about reproductive manifestations in subjects with BV infection in India and specially its effect on fertility. Routinely, the infection is treated only if signs and symptoms are present. 9 To date it is not considered to be a risk factor for reproductive complications in the community. Hence, this study aims to evaluate whether BV infection has any association with different reproductive manifestations. This may highlight the importance of its diagnosis and treatment.
METHODS
Study population
Women attending the Obstetric and Gynaecology Out Patient Department (OPD) of Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital with manifestations such as infertility, recurrent spontaneous abortion (RSA), signs and symptoms of lower genital tract infection (LGTI), and pregnant as well as healthy women without any signs and symptoms of reproductive tract disorder (asymptomatic) were enrolled for the diagnosis of common reproductive tract infections such as BV, candida, trichomonas and two sexually transmitted infections such as Chlamydia trachomatis (C. trachomatis) and human papillomavirus (HPV). Written informed consent as sanctioned by the institutional ethical committees to participate in the study was obtained from each subject before enrolment. Each subject was asked about their reproductive health history, including history of any sexually transmitted infections and current gynaecological symptoms, on a standard clinic form before a pelvic examination. Each woman was asked whether she experienced any increased vaginal discharge with or without a foul smell and itching of the vulva or vagina. Pelvic examination was done to record clinical signs of infection, collect vaginal smear and measure vaginal secretion pH. The diagnosis of vaginitis was made as a part of the routine patient assessment by clinicians, if copious malodorous excessive discharge was present in the posterior fornix. These women were grouped, on the basis of their clinical history and presentation of signs and symptoms, into five groups: (1) women who did not conceive within two years of marriage but were trying to conceive were grouped as infertile; (2) women having a history of two or more repeated spontaneous abortions and did not have any child were grouped as RSA; (3) pregnant women were also screened for infections as antenatal cases (ANC); (4) women having vaginal discharge, cervicitis or vaginitis and with one or more children were grouped as LGTI; and (5) asymptomatic non-pregnant women attending the OPD for family planning advice.
Screening of BV using Gram stain
Vaginal smear was collected with a swab from the posterior fornix after inserting the speculum. A smear for Gram stain was immediately prepared by rolling the swab on the surface of the microscopic glass slide. The material on the slide was fixed by passing through the flame of a burner three times. Vaginal smear was stained with Gram stain (Qualigens Fine Chemicals, Glaxo India Limited, Mumbai, India) and the flora was scored according to Nugent criteria. 10 In brief, for Nugent criteria calculation, each Gram-stained smear was evaluated for different morphotypes under oil immersion (×1000 magnification). Each morphotype was quantified from 1 to 4 with regard to the number of morphotypes per oil immersion field. The absence of lactobacillus morphotype yields the highest score of 4, whereas the presence of more than 30 lactobacillus morphotypes yields a score of 0. Small Gram-variable rods (G. vaginalis morphotypes), small Gram-negative rods (Bacteroides species) and curved Gram-variable rods (Mobiluncus) were quantified from 1 to 4+ with regard to the number of morphotypes per oil immersion field (0, no morphotypes; 1+, less than 1 morphotype; 2+, 1 to 4 morphotypes; 3+, 5 to 30 morphotypes; 4+, 30 or more morphotypes). The scoring criteria summed the weighted quantitation to yield a score of 0–10 for each person. The criterion for BV was a score of 7 or higher; a score of 4–6 was considered intermediate or disturbed flora, and a score of 0–3 was considered normal. For those with an intermediate score, the clinician per speculum observations were taken into consideration to decide the presence of infection and the treatment. In Gram stain, the scoring curved rod morphotype was given less weight because of its lower prevalence and because it was seen as part of an end-stage process in patients with BV. Gram stain has been used as the gold standard for diagnosis of BV, because of its higher sensitivity 11,12 and reproducibility (r = 0.82). 9
Screening of other infections
Wet mount was used to detect candida and trichomonas. Polymerase chain reaction was used to diagnose C. trachomatis and HPV infection. 13,14 Women with any of these infections, except for BV, were excluded from the study as they might influence adverse reproductive outcomes.
Statistical analysis
The Mantel–Haenszel χ2 test was done to study the association of infection with manifestation using Epi Info version 6 packages. Relative risk and odds ratio were used for comparison among women with BV and those with normal vaginal flora. The test of significance for proportion between different groups was carried out using the Z test.
RESULTS
Five hundred and ten women in the age group of 19 to 47 years fulfilled the inclusion criteria during the period of the study. There were 112 (21.96%) women with infertility, 115 (22.5%) women with RSA, 100 (19.6%) women with LGTI, 102 (20%) normal pregnant (gestational age 2–3 months) women attending for ANC and 81 (15.9.%) asymptomatic non-pregnant women attending the OPD for family planning advice. BV was detected in 72 (14.1%) women. The mean age of these infected subjects was 27.7 ± 5.2 years. Age-wise distribution showed a significantly (P < 0.01) high number of infected subjects between 21 and 30 years of age (Figure 1). The clinical history and manifestations of these BV-infected cases were analysed to establish the prevalence of BV infection in different groups (Figure 2). The infection rate was highest (25.9%, 29 of 112) among the infertile women. Infertility was the major/significant associated manifestation followed by RSA. Clinical manifestations associated with these infected subjects, either with single infection or with other infections, were analysed to evaluate the associated sequelae (Figure 3). Associated infections such as candida, C. trachomatis and HPV were observed in 4.16%, 15.27% and 8.33% of BV-infected women, respectively. Co-infection present in each group of BV-infected subjects is presented in Table 1. These infected subjects were mostly asymptomatic (Figure 4). High vaginal pH was recorded in 69 (95.8%) subjects with BV infection. Analysis of clinical manifestations of the remaining 438 women without any infection and its comparison with BV-infected women established the contribution of BV infection towards the development of infertility (Table 2).
Other infections in BV-infected subjects with different clinical manifestations
(%): With reference to total BV infection present in that group
Frequency of clinical manifestations with or without BV infection
PF: Protective factor, EF: Aetiological factor, OR: Odds ratio
χ2: Chi-Square
RSA: Repeated spontaneous abortion
ANC: Antenatal cases
LGTI: Lower genital tract infections
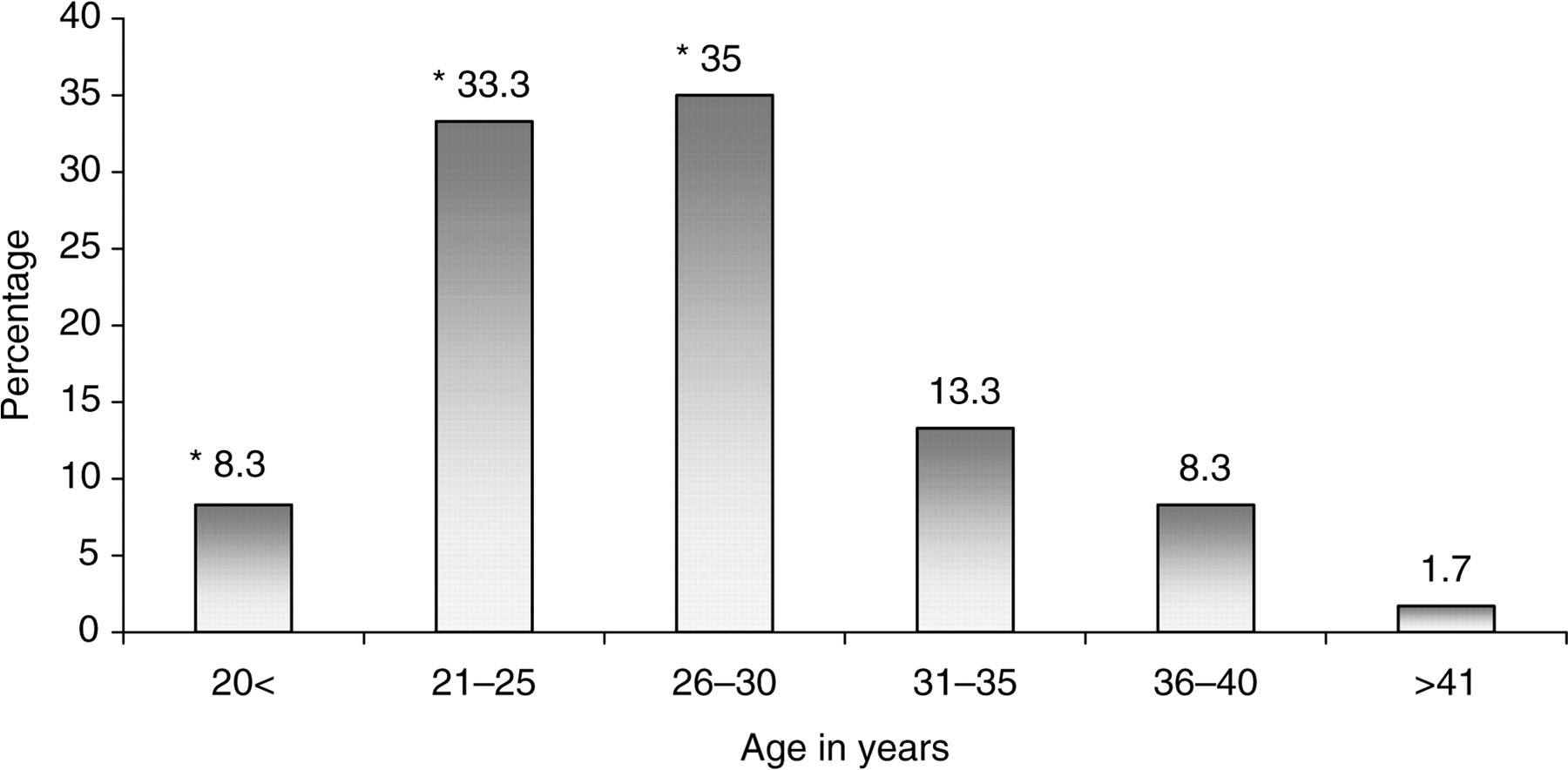
BV infection rate in different age groups. *Z = 3.33; P < 0.01. BV = bacterial vaginosis

Prevalence of BV in women with different clinical manifestations. BV = bacterial vaginosis; RSA = recurrent spontaneous abortion; ANC = antenatal case; LGTI = lower genital tract infection
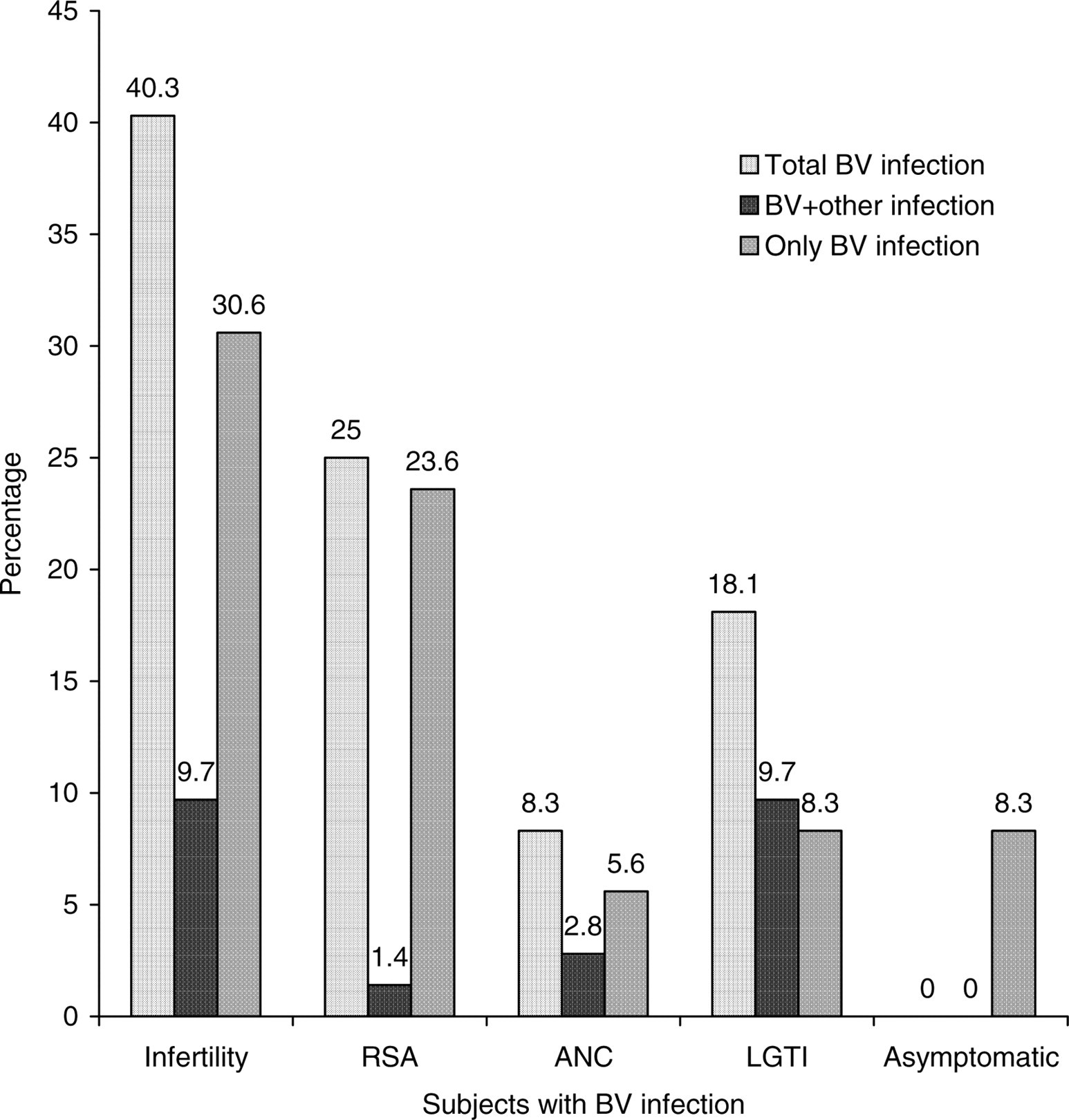
BV and multiple infections rate inwomen with different clinical manifestations. BV = bacterial vaginosis; RSA = recurrent spontaneous abortion; ANC = antenatal case; LGTI = lower genital tract infection
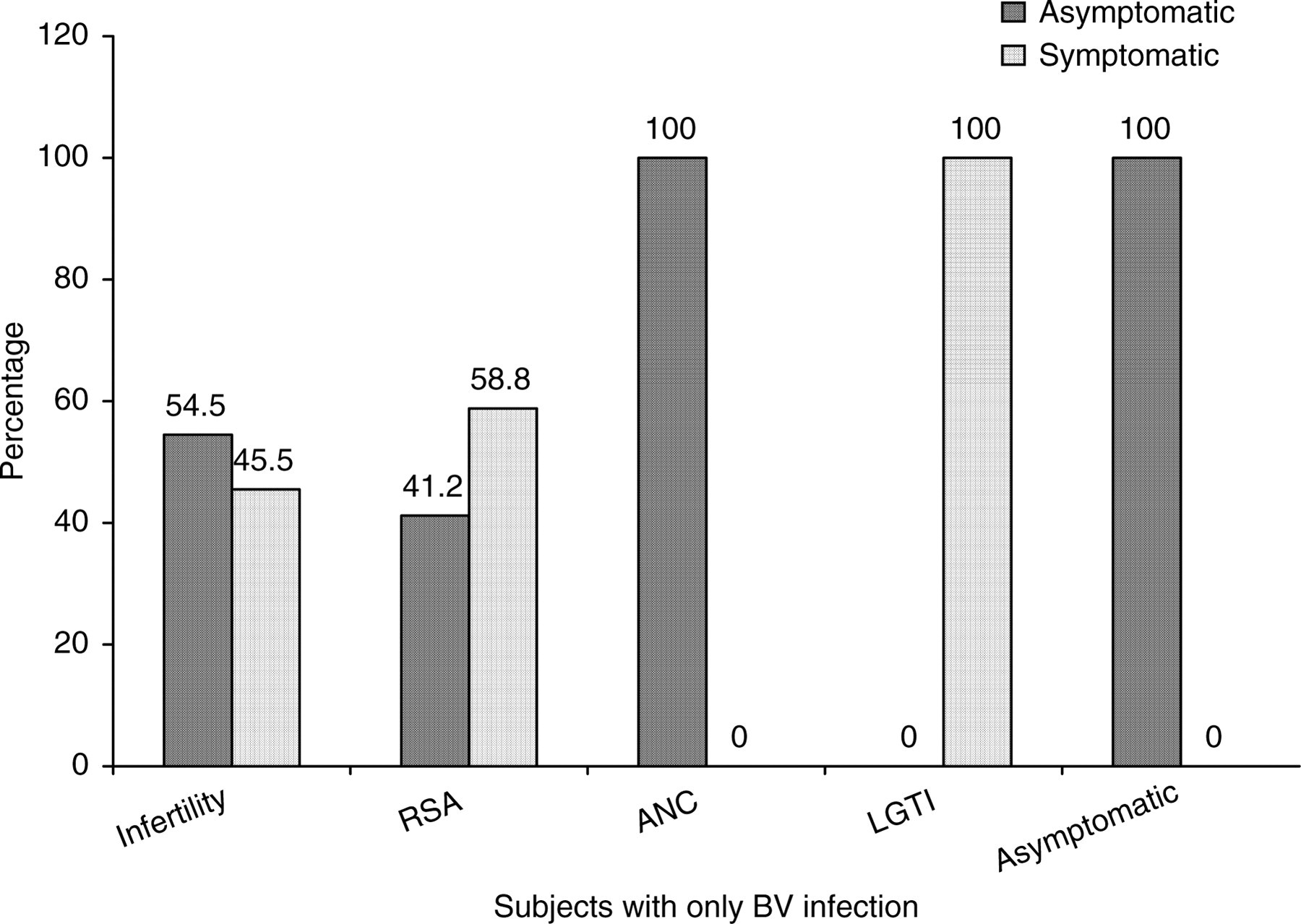
Symptoms and signs present in different groups of BV infected women. BV = bacterial vaginosis; RSA = recurrent spontaneous abortion; ANC = antenatal case; LGTI = lower genital tract infection
DISCUSSION
The prevalence of BV in the study population was 14.1%, which well correlated with a previous study conducted in Mumbai where the infection rate of BV was 13% (58/446). 15 Infection rate was high among women of the 21–35 years age group, which might be due to an active sexual life among infertile women and women with RSA in order to have a successful pregnancy. Little is known about the incubation time of BV. It is possible that women became infected earlier, but it manifested clinically much later. At times this infection also goes unnoticed by affected women. All of this has a strong impact on how physicians view the risks of asymptomatic BV. Most of the infected subjects had a high pH of vaginal secretion, although one previous study has shown that vaginal fluid pH can predict BV infection in 73.4%. 16
In our study, the prevalence rate of BV infection among pregnant women was statistically low. This may be due to multiple factors. It either could be due to pregnancy acting as a protective factor that inhibits this infection or may indicate conception is high in the absence of infection. A similar rate of infection among pregnant women has been documented by Morgan et al. 17 The hormonal changes in pregnancy favour an increase in the concentration of lactobacilli and thus might also favour the elimination of BV. 18 Secondly, BV is more common in sexually active than in non-sexually active women. A reduction in the frequency of intercourse during pregnancy might contribute to a diminishing prevalence of BV. 19
An abnormal cervical–vaginal microflora is associated with adverse pregnancy outcome. 1 It is also reported that the pathological process of BV may begin early in pregnancy and hence does not affect conception, but is associated with an increased risk of miscarriage in the first trimester in women. 20 In the present study, although the prevalence of BV was significantly high in women with RSA as compared with the controls, it cannot be concluded that BV was the aetiological factor for the abortion, since the smear was done after the abortion. However, it would be useful to screen for BV during pregnancy in women with a previous history of spontaneous abortion.
A previous study had shown a significant high infection rate of BV in women with tubal factor infertility compared with those with other causes of infertility. 21 However, it did not show whether this increased BV rate is secondary to previous tubal damage initiated by other infections. Other studies also reported an 18.5% (n = 199) to 25% (n = 120) infection rate in women attending the infertility clinic as compared with only 8.5% of infection in 1379 pregnant women. 17,22 In the present study, we show a statistically significant association between BV infections with infertility than those without this infection, even in the absence of any other infection. Although C. trachomatis infection is known to be associated with infertility, 23 only three of these 29 women had co-infection with C. trachomatis, where they might have played a synergistic role. Immunity to infection might be correlated to sperm rejection in this group of women, leading to infertility that needs further study.
The diagnosis and treatment of BV is simple, cost-effective and would definitely help in improvement of the reproductive health of women in the community, if used as a screening test. Further intervention study may help in assessing whether its treatment reduces reproductive complications such as infertility and pregnancy loss.
Footnotes
ACKNOWLEDGEMENTS
We acknowledge the technical support partly provided by Mrs Shobha Sonawane.