
Abstract
The incidence of Neisseria gonorrhoeae (NG) in Tel-Aviv district, Israel has increased since the mid-1990s. This study aimed to address behavioural attributes and identify the sources of NG infection. Of 1234 NG cases in men reported between 2000 and 2004, 379 (31 %) were interviewed. Most were single, heterosexual and Israeli-born. Insertive oral sex (OS) was reported by 77% patients and vaginal intercourse by 69%, where condoms were used by 4% and 40% for these practices, respectively. Unprotected OS was performed by 95% of the 151 men involved in protected vaginal sex. OS was the most common practice among the younger age group, and in sexual contacts with casual partners or commercial sex workers (CSWs): behaviours that were reported by 37% and 36% of patients, respectively. Unprotected OS is a common route for NG transmission, and it is suggested that the rise in NG may be attributed to unprotected OS with casual partners or CSWs.
Introduction
Neisseria gonorrhoeae (NG), as well as other sexually transmitted infections (STIs) such as syphilis, herpes simplex and human papilloma virus, can be transmitted by unprotected oral sex (OS; fellatio).1–3 A recent study performed in Tel-Aviv district found that 9% of all commercial sex workers (CSWs) tested were infected with pharyngeal gonorrhoea. 3 Due to the asymptomatic nature of pharyngeal NG infection, the patient may be unaware of his/her risk for onward transmission to other sexual partners. The limited public awareness regarding the risks involved in OS and the relative lower intimacy involved in OS compared with vaginal or anal intercourse may promote fellatio. In addition, OS is a popular sexual practice as it is safe in terms of conception risk.
The annual incidence rate of NG in Israel increased from three to 18 cases per 100,000 population between 1995 and 2000. 4 The rise during that period was even more substantial in Tel-Aviv district, increasing from 1.3 to 27.3 per 100,000 population. 5 The incidence of NG in Israel is still lower than in other industrialized countries, such as Australia, 6 Canada, 7 UK 8 and the USA,9,10 during the same period (15, 30, 35 and 125 per 100,000 population, respectively). However, in light of the increasing trend of NG infections in Tel-Aviv district, appropriate containment measures are required to control infection.
Tel-Aviv district is the major metropolitan area in Israel, housing 1,176,000 residents, of whom 67% are aged below 50 years. Tel-Aviv also serves as the commercial capital of Israel, with an additional 1,613,700 citizens living in the districts surrounding it, of whom more than 500,000 commute to Tel-Aviv daily. 11 Like other big cities, Tel-Aviv offers a wide variety of premises in which sexual activities are performed, such as brothels, night clubs, ‘pick-up’ bars and public venues where sexual activities are performed. During the last decade, the female CSW population in Israel has been augmented by immigrants, mainly originating from eastern European countries.3,12,13
In the face of increasing NG incidence and the changing composition of CSWs in Tel-Aviv district, we conducted a study among patients diagnosed with NG to assess behavioural risks and to identify the source of infection. The findings of this study can be used to guide behavioural interventions to decrease STI morbidity.
Methods
NG is a notifiable disease in Israel. Physicians and laboratories are independently required to report cases individually to the district health department, including demographic attributes, such as the patient's age, sex, address and telephone number. NG notifications are also required from physicians in cases where they suspect the diagnosis on clinical grounds and microscopic examination of urethral discharge detecting diplococci.
The health department conducts epidemiological investigations for communicable diseases in order to prevent further infections and to detect the sources of infections. Due to the increased incidence of NG in Tel-Aviv district, all patients infected with NG who lived in Tel-Aviv district were sent a letter inviting them for an interview at the health department. In those cases where the patient did not respond to the first letter, a second invitation was issued. The interviews were performed by the attending physicians at the health department, using a structured questionnaire, including information on the patient's demographic details, clinical symptoms, sexual behaviour, type of sexual partner (steady partner, friend, casual contact or CSW), history of paying for sex and condom use. Participants who answered yes to the question regarding condom use were categorized as ‘condom users’. Incomplete or negative responses regarding condom use were categorized as ‘condom non-users’. Sexual orientation was not asked about explicitly; yet, patients were free to discuss the issue with the physicians.
This study presents the summary of the epidemiological investigations performed between January 2000 and December 2004. As most of the patients (92.4%) reported to the health department were men, we focused our analysis on urethral NG in male patients only.
Comparisons between categorical variables were computed using the chi-square or Fisher exact tests when indicated, and comparisons between continuous variables were performed by the Student's t-test for variables distributed normally and by the Mann–Whitney test for variables that were not normally distributed. P < 0.05 was considered significant. Analyses were performed using SPSS package version 13.0 for Windows software (SPSS Inc, Chicago, IL, USA).
Results
During the study period 1335 individuals infected with NG were reported to the Tel-Aviv health department, representing an average annual incidence of 22 cases per 100,000 population. Men comprised 92.4% of this cohort (Figure 1). Of all 1234 men who were invited for interview, 379 (31%) attended, 467 (38%) did not and 388 (31%) could not be located (wrong postal address).
Total numbers and incidence rates of Neisseria gonorrhoeae infection reported in Tel-Aviv district, by sex, 1995–2004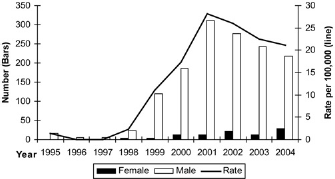
The characteristics of the interviewed male patients were similar to those of total male patients reported to the Tel-Aviv health department: the mean age of the patients interviewed was comparable with the mean age of all 1234 male patients reported in Tel-Aviv district (32.6 ± 9.8 and 31.2 ± 9.5 years, respectively). The geographical distributions of men interviewed were similar to that of all male patients in Tel-Aviv district (central and southern towns, east towns, north towns distributions were 68.1%, 26.8%, 5%, and 68.5%, 27.4%, 4.2%, respectively).
Symptoms described by men with urethral NG included urethral discharge (93%) or burning (83%), dysuria (10%), dyspareunia (7%) and genital ulcer (3%). Diplococci were identified in 20% of smear samples and the cultures were positive in 61%. All other cases reported were based on clinical diagnosis.
Most interviewees were single, young Israeli-born men (Table 1). Of the non-Israeli-born patients, the patients who were born in the Former Soviet Union had been residing in Israel for an average of 12 ± 9 years, while those who were born elsewhere had been living in Israel for significantly longer periods (39 ± 12 years, P < 0.01). The most frequently affected age group was 22–30 years (42.4%). Of the 304 who responded, the average years of education were 12.5 ± 2.2 (range 6–22). Any previous STI (gonorrhoea, syphilis and hepatitis B) was reported by 80 (21%) patients, more commonly in men aged 34 or older than in the younger age group (30.8% versus 15.6%, P > 0.01).
Demographic characteristics of interviewed male patients infected with urethral Neisseria gonorrhoeae in Tel-Aviv district, 2000–04

Most men reported they had sexual contact with women, while 25 (6.6%) were men who had sex with men (MSM). The most likely sexual encounter for NG acquisition as described by men who had sex with women was either a casual partner (36.6%) or a CSW (35.%), while 15.5% suspected a friend and 12.1% indicated their steady partner might have been the source.
Insertive OS was the most frequent sexual practice reported by men (77.3%), followed by vaginal sex (VS) (68.6%). Condoms were used more commonly for VS than OS (39.8% versus 4.2%, respectively, P < 0.01) (Figure 2). Unprotected OS was reported by 95% of 151 male participants who had practised protected VS.
Sexual practices and condom use by male patients with urethral Neisseria gonorrhoeae infection in Tel-Aviv district, 2000–2004
Study participants who used condoms during VS had more unfamiliar sexual partners (either casual or CSW) than non-users (80.8% versus 50.5%, respectively, P < 0.01). No significant association was found between condom use during VS and patient's age (P = 0.06), education level (P = 0.9), marital status (P = 0.3), country of origin (P = 0.6), and length of stay in Israel for the non-Israeli-born patients (P = 0.3), past NG infection (P = 0.5) or with condom use for OS (P = 0.1).
Education level was associated with particular sex practices: patients with higher levels of education (13 years or higher) reported OS more commonly than those who had lower levels of education (87% versus 76%, respectively, P = 0.05). In contrast, patients with lower levels of education (12 years or lower) reported more VS than those of higher education (74% versus 61%, respectively, P = 0.03).
Table 2 describes the demographic and behavioural characteristics of NG-infected men who had sex with CSWs compared with those who did not. A greater percentage of men who had sex with CSWs were married, older than 34 years and non-Israeli-born in comparison with those who did not pay for sex. Condom use for VS was significantly more frequent among those who had sex with CSWs than those who did not pay for sex. Those who paid for sex received OS more commonly than those who did not pay for sex and no significant differences were found in condom use between the two groups.
Demographic and behavioural characteristics of urethral Neisseria gonorrhoeae-infected male patients by use of CSWs, 2000–04
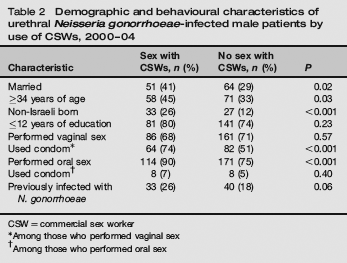
CSW = commercial sex worker
Among those who performed vaginal sex
Among those who performed oral sex
Same sex practices were reported by 25 MSM, who indicated more frequent anal sex (AS) than those who had sex with women (36% versus 0.6%, respectively, P < 0.01). Seventeen (68%) MSM suspected they were infected by a casual sexual partner, five (20%) suspected a friend and three (12%) indicated that their regular partner might have been the source. Most MSM (24, 96%) had OS during their encounter and did not use condoms.
Discussion
Most interviewed patients infected with urethral NG were men who declared they had sex with women and reported unprotected OS with a CSW or a casual partner. This study therefore suggests that pharyngeal infection may serve as a reservoir for transmitting NG to the urethra during fellatio.
Insertive OS was the most common practice described by men, regardless of their place of birth, age and marital status. Condom use during OS was minimal. The asymptomatic nature of pharyngeal gonorrhoea may delay referral to medical services, resulting in a late diagnosis and treatment. The increasing popularity of OS might be explained by its perception as a low-risk practice for the acquisition of STIs, HIV infection or conception, 14 especially among MSM and young individuals, and is perhaps regarded as less intimate than other sexual practices, such as VS or AS. 15 OS was the most commonly reported practice with CSWs, as it can be performed in the client's car or in public areas, and is normally cheaper compared with VS, which also requires a different setting. In another study performed in Tel-Aviv district in 2001, pharyngeal NG was detected in 9% out of 301 CSWs. 3 This high rate of pharyngeal NG infection among CSWs along with the limited use of condoms during fellatio reported by patients in our study who did use a condom during VS may explain NG infection in men who had OS with a CSW.
The younger age group may use fellatio as a strategy for safer sex than VS or AS in regard to HIV acquisition, undesired pregnancies and preservation of virginity. 16 In a report from the UK, fellatio was reported by 78% of both men and women in the preceding 12 months in the age group 16-44 years, 17 predominantly by younger individuals. Another study among high school students performed in the UK 18 found that less than 22% used condoms during OS, and no difference was found in condom use between those who knew fellatio posed a risk of STI and those who did not. 19 Similar findings were also reported from the USA. 20
Fellatio is a common practice, especially among CSWs, MSM and in young, urban individuals,21,22 all of whom are considered at high risk for STI acquisition. Therefore, stronger emphasis should be made by health educators to convey the risk of OS as a possible route for STI transmission and to encourage condom use during fellatio with a casual or paid partner. 23 The most common reasons provided for not using condoms during OS in studies were its unpleasant taste, throat itchiness and the loss of sensation. 22 Therefore, distributing flavoured, thin condoms may help overcome such barriers. 24 Among CSWs, especially those emigrating from other countries, interventions should be employed to improve negotiation skills and to increase condom use when performing OS. Such efforts should also engage brothel keepers and CSW peers. 24 Additionally, as pharyngeal NG infections may be asymptomatic, appropriate routine screening and early treatment should be considered in high-risk populations.
Due to the increased incidence of NG in Tel-Aviv district, a designated clinic targeting CSWs was established by the Ministry of Health in Tel-Aviv in 2002. From 2004 onward, a mobile van adjoined the clinic service, providing outreach to high-risk individuals in brothels and in the streets and offering anonymous testing and free therapy, including pharyngeal swabs for NG culture. Nevertheless, while employing risk reduction strategies in our clinic, we promote condom use for OS only secondary to the use of condoms during VS and AS practices, which are more conducive routes for NG, HIV and other STIs.
Condom use habits among Israeli-born patients were not different from those of the non-Israeli-born, regardless of their length of stay in Israel. Our findings are inconsistent with reports published from other countries, indicating riskier sexual behaviour among immigrants compared with locals.21,25,26 This inconsistency may be partially related to the unique fashion of immigration to Israel, where the majority of immigrants arrive legally and for permanent settlement, unlike foreign work labourers in other developed countries, who may arrive temporarily. Immigrants to Israel usually arrive with their families rather than alone, thus practising similar sexual behaviour as married Israeli-born individuals. We also believe that there was little reporting bias among migrants, as they are fully medically insured upon arrival and are able to seek medical care as Israeli citizens do.
Those who used CSWs in our study were more likely to be married, older and of non-Israeli origin than those who did not pay for sex. These findings are in line with previous studies performed among sex work clients in developed countries.27–29 Married men could transmit the infection to their concomitant steady partners (‘bridging’), such as their spouses, who are normally considered a lower-risk population. The rate of condom use for VS with CSWs in our study was significantly higher than for OS, yet was still suboptimal. A focused health campaign for those married men may help decrease the spread of NG in the community.
The study is subject to potential limitations. First is the low response rate for the invitation to be interviewed at the health office. Nevertheless, patients who completed the interview were similar to the entire cohort of NG patients in Tel-Aviv district by age, gender and place of residency. Second, STI history taking may also be subject to both reporting and recall bias, which may affect the reliability of the responses completed by the interviewees. For example, a patient may feel more comfortable to ‘blame’ the CSW for his gonococcal infection or may recall more significantly the paid sex event rather than a previous encounter with an acquaintance. Third, interviewees were not explicitly asked about sexual practices with other men, although the interviewers could lead the conversation in this direction if desired. Lastly, a high male to female ratio existed in the entire cohort of NG-infected patients. This can be supported by the fact that a high proportion of NG-infected women are asymptomatic, while most men develop symptoms and therefore seek medical care.30,31
As we acknowledge that the results of this study may not be generalized to all NG patients in Israel, this is a relatively large study of male NG patients interviewed in Israel, which includes behavioural attributes and clinical data. Thus, it can make a substantial contribution to the current body of knowledge in identifying individuals at risk for infection and guide future focused health intervention campaigns.
In conclusion, most patients with NG infection in our study were men who reported sexual contact with a female CSW or a casual partner, where OS was the most common practice. Further prevention interventions should promote behavioural change and increase awareness of the risks of NG transmission during fellatio, including MSM, CSWs and their clients. Those interventions should be evaluated by larger nation-wide studies.
Footnotes
Acknowledgements
The authors would like to thank the following physicians for interviewing the patients and for completing the questionnaire at the Tel-Aviv department of health, Dr Lea Serbu, Dr Rivka Sheffer and Dr Matthew Lewis, and also Ms Margalit Softer for her logistic assistance.