
Abstract
We identified demographic, clinical and biological determinants of herpes simplex virus type 2 (HSV-2) shedding among HIV-infected participants in the Women's HIV Interagency Study (WIHS). Cervicovaginal lavage (CVL) specimens from 369 HIV-infected HSV seropositive women were tested with TaqMan polymerase chain reaction (PRC) for detection HSV-2 DNA. Seven percent of women tested positive for HSV-2 DNA in CVL. Significant correlates of the presence of HSV-2 DNA in CVL were being younger, African American or Hispanic race/ethnicity and injecting drugs in the past six months (P < 0.05). A borderline significant trend for reduced viral shedding with higher CD4+ T cell counts was observed (P = 0.08). All women who were never observed with any genital lesions and had consistently negative self-reported history of genital sores throughout the follow-up (n = 29, 8%) were negative for CVL HSV-2 DNA. HSV-2 DNA quantity was significantly associated with having frequent subsequent lesion recurrences (Spearman rho = 0.48, P = 0.016; adjusted prevalence ratio [APR] = 2.5, P = 0.012). Increasing the age of the host was inversely correlated with decreased viral shedding over time. However, a subset of older women continued to shed significant amounts of virus despite passage of time. This study provides genital HSV-2 DNA titre as a quantitative and symptom- and sign-based measures as qualitative predictors of HSV-2 shedding from the lower genital tract among HIV-infected women.
Introduction
Herpes simplex virus type 2 (HSV-2) infection is the most common aetiology of genital ulcer disease in the world and a risk factor for human immunodeficiency virus (HIV) infection.1–4 After much research on HSV-2, the determinants of genital herpes (GH) course and factors affecting reactivation rates are still not well defined. Over 90% of individuals with antibodies to HSV-2 are asymptomatic and unaware of their infection 5 and only a small proportion present with classical symptoms of recurring painful vesicular lesions with enlarged regional lymph nodes after a symptomatic primary or a first clinical episode. Close investigation of HSV-2 seropositive but asymptomatic individuals has revealed that many of them experience various symptoms but fail to recognize these as related to HSV-2.6–10 More than 50% of individuals with unrecognized HSV-2 shed the virus genitally. Importantly, at least 70% of transmissions may occur during these unrecognized reactivations.11,12
Therefore, it is important to identify factors that predict shedding and how shedding changes over time, particularly among HIV-infected individuals in whom HSV-2 is highly prevalent and associated with increased HIV replication and disease progression.13–19 This study was conducted within the Women's Interagency HIV Study (WIHS), the largest ongoing cohort study of HIV among women in the USA. Specific aims were to explore: (1) whether HSV-2 DNA titre can serve as a virological correlate for HSV-2 course and (2) demographic, risk and clinical correlates of genital HSV-2 shedding. Identifying and characterizing these correlates could be valuable for targeted identification, timely testing and proper management of HSV-2 in HIV-infected women.
Methods
Study population
The study population consisted of HIV-infected women from the WIHS. Details of the study population have been described elsewhere.20,21 WIHS enrolled 2059 HIV-infected and 569 uninfected women from October 1994 to November 1995. Women underwent clinical evaluations with a collection of biological specimens every six months with a detailed questionnaire administered by an interviewer.
Specimens and laboratory procedure
Serological reactivity to HSV-1 and HSV-2 was determined by glycoprotein G-based enzyme immunoassay (gG-EIA; Gull Laboratories, Salt Lake City, UT, USA). Negative and equivocal results were confirmed by Western blot as previously described. 13 Gynaecological examination included assessment for genital tract infections, including ulcers and intraepithelial dysplasia as previously described. 22 Clinicians’ assessment of GH was based primarily on visualization of ulcers and/or vesicles in the genital area during pelvic exam and viral culture when a primary outbreak was clinically suspected. Interval history of genital sores was collected by self-report at each study visit. Women were scheduled for visits when they were not menstruating and were instructed to avoid inserting any substance into the genital tract for 48 hours before their examination. 23
Cervicovaginal lavage (CVL) samples from 369 HIV-infected HSV-1 and/or HSV-2 seropositive women were retrieved from the WIHS repository for testing with duplex quantitative realtime TaqMan polymerase chain reaction (qPCR) for HSV-1 and HSV-2 DNA. Details of the qPCR assay were described elsewhere. 24 Briefly, HSV DNA was detected using 200 μL of whole CVL. CVL specimens were collected by flushing the cervix with 10 mL sterile normal saline. Primers amplified a 155–nucleotide region of glycoprotein B (gB) envelope gene homologous for HSV types 1 and 2. Commercial HSV-1 or HSV-2 quantitated DNA (ABI Advanced Technologies, Inc, Columbia, MD, USA) was used to establish the standard curve. Specimens were run in duplicate and were considered positive if HSV DNA was detected in both replicates.
To explore whether the baseline HSV-2 DNA titre could serve as a virological correlate for subsequent HSV-2, selection was restricted to women with at least one follow-up visit since the baseline, who had multiple recurrent lesion-episodes (L-Es) (>2 visits with genital lesions during follow-up) and more than 5 mL of CVL available to preserve the specimens. Each woman contributed a single specimen from the first available L-E. Eighty percent of tested specimens were collected in the first 4.5 years of the study, prior to widespread use of highly active antiretroviral therapy (ART).
Statistical analysis
Uni- and multivariate log-binomial and their Poisson extensions 25 were used to determine crude and adjusted prevalence ratios (APRs) for associations of interest. Plasma HIV RNA load was dichotomized at 4000 copies/mL. Ordinal categorical variables were modelled as continuous variables to test for linear trends. Lowess smoothing graphs were used to visually display the trends and associations. All analyses were performed using Stata 10.1 (Stata Corp, College Station, TX, USA).
Results
Demographic and risk characteristics of the study population
The study population consisted of 369 HIV-infected women (Table 1). Over 80% were HSV-2 seropositive at baseline. Age, race and risk factor distributions were reflective of the corresponding distributions in the WIHS population.
Baseline demographic and risk characteristics of 369 HIV-infected study participants
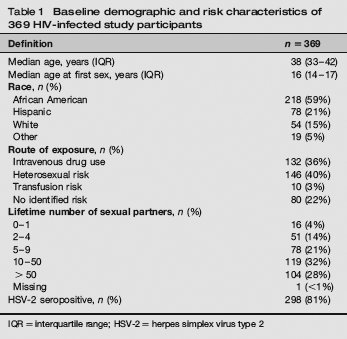
IQR = interquartile range; HSV-2 = herpes simplex virus type 2
qPCR results
Overall, the single time point prevalence of HSV-2 DNA positivity in CVL was ∼7% (n = 25). No HSV-1 DNA was detected.
Clinical indicators of HSV-2 infection as correlates of HSV-2 shedding
HSV-2 seropositivity, presence of any lesions and lesions clinically suspected to be herpetic were associated with a ∼3–5 times higher probability of the presence of HSV-2 DNA in CVL compared with HSV-2 seronegative women and those with no lesions (Table 2). Additionally, a composite indicator was created that combined sign- and symptoms-based indicators into ever/never present over the duration of a woman's follow-up. If a participant had a positive history of GH sores or had any lesions at least once during her follow-up, she was considered positive for the composite indicator or symptomatic and was considered negative for the composite indicator or asymptomatic otherwise. Using this definition, all 25 women positive for CVL HSV-2 DNA were symptomatic at least once during the follow-up and all women negative for the composite indicator or who were never observed with any genital lesions and had consistently negative self-reported history of genital sores throughout the follow-up (n = 29, 8%) were negative for CVL HSV-2 DNA.
Detection of HSV DNA in CVL by clinical indicators of HSV-2 infection

HSV = herpes simplex virus; CVL = cervicovaginal lavage; GH = genital herpes;
CI = confidence interval
(+) condition present; (–) condition absent
Any genital lesions including not diagnosed as herpetic versus no lesions
Lesions clinically suspected as herpetic versus other lesions
Composite indicator of GH self-report, any lesions or herpetic lesions versus those not reporting either of them over the duration of follow-up
Prevalence ratio was not calculated due to 0 frequency in the cell
Association of the CVL HSV-2 DNA load with the number of subsequent L-Es observed during follow-up
A positive correlation was observed between HSV-2 DNA titre in CVL and the subsequent number of genital L-Es (Spearman rho = 0.48, P = 0.016). There was no correlation between the length of follow-up time and HSV-2 DNA titre in CVL (Spearman rho = –0.07, P = 0.725), indicating that this association was not due to varying lengths of follow-up times. The increase in HSV-2 DNA copy number was more pronounced for women with >4 subsequent L-Es (Figure 1). Therefore, regression analyses were performed with the proportion of >4 L-Es as a dichotomous outcome using data from women with >4 follow-up visits (n = 19). In this analysis, the crude pre-valance ratio (PR) was 1.5 (95% confidence interval [CI]: 1.1–1.9, P = 0.009) and APR from multivariate analysis adjusted for age, age at first intercourse, race, use of ART, HIV RNA category and CD4+ T-cell count was 2.5 (95% CI: 1.2–5.2, P = 0.012).
Lowess smoothed graph of herpes simplex virus type 2 viral titre in genital secretions by total number of subsequent visits with genital lesions observed during follow-up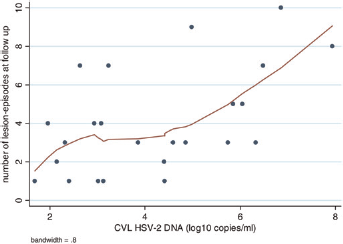
Association of demographic, risk exposure factors and HIV disease markers with HSV-shedding
Younger, African American and Hispanic women and women who had injected drugs in the past six months were three to five times more likely to shed HSV-2 as compared with women who were older, of other race/ethnicity and who had not injected drugs in the past six months (P < 0.05, Table 3). A borderline significant trend for reduced probability of HSV-2 shedding with higher CD4+ T-cell counts was observed (P for trend = 0.08).
Association of demographic, risk factors and HIV disease markers with cervicovaginal shedding of HSV-2 among 369 HIV-infected women
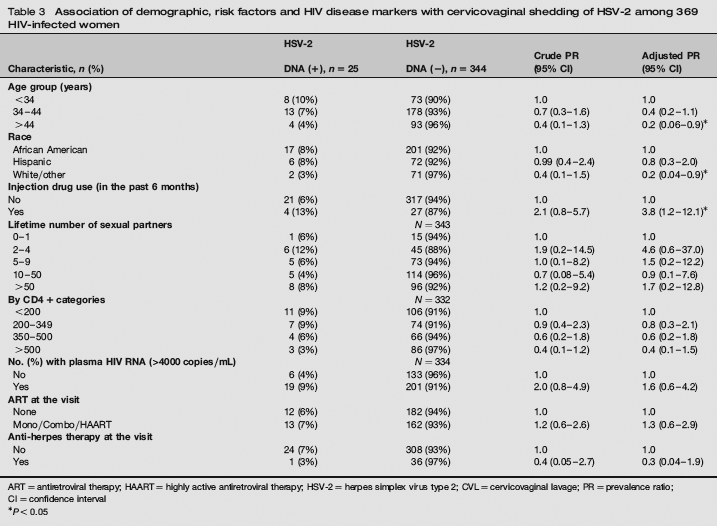
ART = antiretroviral therapy; HAART = highly active antiretroviral therapy; HSV-2 = herpes simplex virus type 2; CVL = cervicovaginal lavage; PR = prevalence ratio;
CI = confidence interval
P<0.05
The above results are consistent with the data observed in the entire cohort. Specifically, the decline in CVL HSV-2 DNA detection with age was consistent with the decline in the occurrence of lesions observed during the follow-up in both HIV infected and uninfected women (Figure 2). Among HIV uninfected women (n = 63) only two (3%) were positive for HSV-2 DNA, thus restricting our ability to study correlates of HSV-2 shedding in this group. Nevertheless, the two-fold greater proportion of HSV-2 DNA detection in CVL among HIV-infected women was consistent with the two-fold greater occurrence of lesions compared with HIV-uninfected women.
Lowess smoothed plot of occurrence of genital lesions and clinical genital herpes episodes over study visits by HIV infection status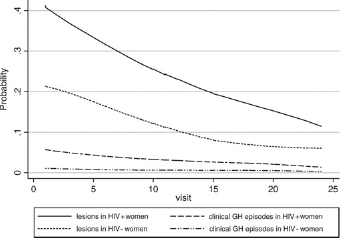
Discussion
This study identified several correlates of HSV-2 shedding among HIV-infected women. Two of these correlates may be useful in clinical practice and deserve further study. First, the study found a positive correlation between the CVL HSV-2 DNA load and the number of subsequent L-Es, which suggests that the titre of viral shedding in genital secretions may be a useful prognostic factor for the recurrence of clinical reactivations, i.e. determining the course of GH. To date, data on the association between genital HSV-2 viral titre and the course of HSV-2 have been limited. One study, for example, found that first episodes of GH were associated with higher viral loads compared with recurrent (4.2 × 105 copies per reaction versus 1.0 × 104; P = 0.0002). 26 More recent study observed persistent long-term viral shedding but trend for reduced titre of viral shedding over time. 27 Thus, these results support the previously suggested notion of establishing a viral set point concept in HSV-2 pathogenesis.
Second, the composite measure of the long-term occurrence of the signs and symptoms of HSV-2 reactivation may be useful in distinguishing those potentially shedding the virus from those who are not, since none of the women negative for the composite indicator were positive for HSV-2 DNA. As the median follow-up time of participants was 10 years, further studies are needed to confirm this finding and to determine the minimum time frame necessary to be negative for clinical signs and/or symptoms of HSV-2, to exclude the risk of shedding.
In addition, this finding has potentially two other implications. First, it appears that there is a subset (albeit small) of individuals who, despite being HSV-2 seropositive and followed for a long time, were never observed to have any lesions during physical/gynaecological exams and had consistently negative self-reports of any genital sores throughout the follow-up. Second, the fact that none of them were positive for HSV-2 DNA may indicate that these individuals could have controlled HSV-2 infection and are at low risk of shedding. At a time when there is considerable debate about recommending universal HSV-2 serological screening, whether those with serological evidence of HSV-2 need to be given suppressive therapy and whether these actions will have public health or individual benefits, the above evidence may be contributory as it suggests that not everyone who is HSV-1 or HSV-2 seropositive needs screening for genital HSV shedding or HSV suppressive therapy.28–30
The proportion of women shedding HSV-2 decreased as individuals aged, which is consistent with previous studies.10,31,32 Given the older median age of women, early age at first intercourse and the high baseline number of lifetime sexual partners, it is likely that HSV-2 was acquired in the remote past. Yet, more than half of those positive for CVL HSV-2 DNA were aged between 34–44 years and older. Moreover, older participants who were still shedding had higher CVL HSV-2 DNA copy numbers and were more likely to have decreased CD4+ T-cell counts.
The limitations of this study include the relatively low rates of women with detectable HSV-2 DNA in CVL compared with other studies33–36 and the lack of longitudinal measurement of viral shedding. Some factors that possibly contributed to low detection rate include sampling any rather than only herpetic lesions, the longstanding nature of HSV-2 infection in women, likely varying lesional stages at presentation (e.g. crusted lesions may not have yielded the virus), higher CVL dilution factor and the single measurement of HSV-2 shedding.
In summary, this study explored both quantitative (genital HSV-2 DNA titre) and qualitative (clinical sign and symptom based indicators) predictors of HSV-2 shedding from the lower genital tract among HIV-infected women. Higher copy numbers of viral DNA in genital secretions was associated with increased subsequent risk of clinical recurrences. Long-term absence of genital lesions and other signs and symptoms of HSV-2 may be indicative of minimal risk of genital HSV-2 shedding. Younger HIV-infected African American and Hispanic women were at increased risk of HSV-2 shedding. Clinicians and public health practitioners may want to consider these correlates in the management of HSV-2 infections in HIV-infected women.
Footnotes
Acknowledgements
Data in this manuscript were collected by the Women's Interagency HIV Study (WIHS) Collaborative Study Group with centres (Principal Investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, NY (Howard Minkoff); Washington, DC Metropolitan Consortium (Mary Young); The Connie Wofsy Study Consortium of Northern California (Ruth Greenblatt); Los Angeles County/Southern California Consortium (Alexandra Levine); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange). The WIHS is funded by the National Institute of Allergy and Infectious Diseases (UO1-AI-35004, UO1-AI-31834, UO1-AI-34994, UO1-AI-34989, UO1-AI-34993 and UO1-AI-42590) and by the National Institute of Child Health and Human Development (UO1-HD-32632). The study is co-funded by the National Cancer Institute, the National Institute on Drug Abuse and the National Institute on Deafness and Other Communication Disorders. Funding is also provided by the National Center for Research Resources (UCSF-CTSI Grant Number UL1 RR024131). The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.