
Abstract
Herpes simplex virus type 2 (HSV-2) infection is one of the most common sexually transmitted infections (STIs) worldwide. While glycoprotein G-2 enzyme-linked immunosorbent assays are commonly used for the serological detection of HSV-2 antibodies, they have low specificity in developing countries. The Euroline Western blot (WB) is a commercially available assay that is easy to perform; however, little is known about its performance characteristics. This study evaluated Euroline WB for the detection of HSV-2 antibodies compared with University of Washington Western blot in three geographically different regions: Baltimore, MD, USA; Rakai, Uganda; and Kunming, China. Among the 135 American men attending a STI clinic in Baltimore, MD, 72% (n = 97) were HSV-2-positive by Euroline WB, showing a sensitivity of 97.8% and a specificity of 81.8%. Among the 273 commercial sex workers in Kunming, 62.3% were HSV-2-positive by Euroline WB (sensitivity 96.9%, specificity 89.1 %). Among the 437 Ugandans in Rakai, 67.3% were HSV-2-positive by Euroline WB (sensitivity 98.7%, specificity 65.4%). The Euroline WB has a consistently high sensitivity, but specificity varied significantly among the different locations.
Keywords
Herpes simplex virus type 2 (HSV-2) infection is one of the most common sexually transmitted infections (STIs) worldwide 1–3 and can cause genital ulceration and neonatal infection.4,5 While there are glycoprotein G-2 (gG-2) enzyme-linked immunosorbent assays (ELISAs) commonly used for the serological detection of HSV-2 infections,6–10 they have low specificity in developing countries when compared with the most stringent comparative standard, a Western blot performed at the University of Washington (UWWB).6–9,11–14 However, the UWWB is expensive and difficult to perform. The Euroline Western blot (WB) is a commercially available assay that is easy to perform; however, little is known about its performance characteristics. Therefore, we evaluated the Euroline WB for the detection of HSV-2 antibodies in three geographically distinct regions: Baltimore, MD, USA; Rakai, Uganda; and Kunming, China.
The study utilized previously collected sera from men attending STI clinics in Baltimore, MD, commercial sex workers (CSWs) in Kunming, Yunnan Province of China, and Ugandans in rural Rakai District.6,9,10 The samples were from three distinct populations with varying HSV-2 prevalence.2,15–18 The original studies were reviewed and approved by institutional review boards at the Uganda Virus Research Institute, the AIDS Research Subcommittee of the Uganda National Council for Science and Technology, Yunnan University, Columbia and Johns Hopkins University, and the National Institutes of Health. All assays were performed at Johns Hopkins University, except for the UWWB.
For the detection of HSV-2 antibodies, the Euroimmun anti-HSV-1/HSV-2 gG-2 Euroline-WB (IgG) (Lübeck, Germany) assay was used following the manufacturer's protocol. Euroline WB strips contain electrophoretically separated antigen extracts of HSV-2 and a membrane chip with affinity chromatography-purified HSV-2 gG-2. The strips were evaluated using the Euroline scanner and confirmed by visual examination. The Euroline scanner and computer program called each sample positive, borderline or negative. Borderline strips were considered positive for concordance, sensitivity and specificity calculations.
The sensitivity and specificity of the Euroline WB was compared with UWWB as the comparative ‘gold’ standard. The positive and negative predictive values were not calculated since the sample sets were not representative of the entire population. Samples with atypical UWWB results were considered negative for HSV-2 for analysis purposes. Kappa concordance values, sensitivity and specificity were estimated using Microsoft Excel.
Among the 135 men attending a STI clinic in Baltimore, 72% (n = 97) were HSV-2–positive by Euroline WB and 67.4% by the UWWB. Using the UWWB as the comparative standard, Euroline WB had a sensitivity of 97.8%, a specificity of 81.8% and a concordance of 92.6% (Figure 1). There was no significant improvement in specificity (84.1%) if samples read as borderline by Euroline were considered negative. Among the 273 CSWs in Kunming, 62.3% (n = 170) were HSV-2-positive by Euroline WB and 60.0% by the UWWB. Using the UWWB as the comparative standard, Euroline WB had a sensitivity of 96.9%, a specificity of 89.1% and a concordance of 93.8% (Figure 1). Specificity was 93.6% if samples read as borderline by Euroline were considered negative. Among the 437 Ugandans in Rakai, 67.3% (n = 294) were HSV-2-positive by Euroline WB and 51.0% by the UWWB. Using the UWWB as the comparative standard, the Euroline WB had a sensitivity of 98.7%, a specificity of 65.4% and a concordance of 82.4% (Figure 1). There was no significant improvement in specificity (66.4%) if samples read as borderline by Euroline were considered negative.
Sensitivity, specificity and concordance for the Euroline Western blot assay HSV-2 antibody detection in Baltimore, Kunming and Rakai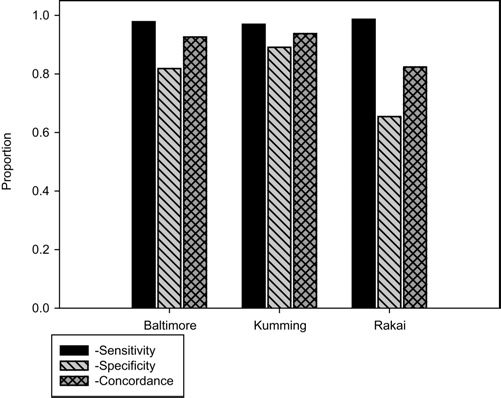
For HSV-1, 68.9% (93/135) men attending a STI clinic in Baltimore were positive by Euroline WB and 91.1% (123/135) by the UWWB. Using the UWWB as the comparative standard, Euroline WB had a sensitivity of 98.9%, a specificity of 26.2% and a concordance of 76.3 %. Specificity improved to 42.9% if samples read as borderline by Euroline were considered negative. Among the CSWs in Kunming, 91.5% (250/273) were HSV-1-positive by Euroline WB and 91.9% (251/273) by the UWWB. Using the UWWB as the comparative standard, Euroline WB had a sensitivity of 98.0%, a specificity of 81.8% and a concordance of 96.7%. Specificity was 90.9% if samples read as borderline by Euroline were considered negative. Among the individuals in Uganda, 88.7% (368/415) were HSV-1–positive by Euroline WB and 93.0% (386/415) by the UWWB. Using the UWWB as the comparative standard, the Euroline WB had a sensitivity of 90.2%, a specificity of 31.0% and a concordance of 86.0%. Specificity improved to 37.9% if samples read as borderline by Euroline were considered negative.
This study represents the largest investigation of the performance of the Euroline WB using samples from three distinct geographic locations. For detection of HSV-2, we found that the Euroline WB has a consistently high sensitivity (96.9–98.7%), but specificity varied significantly among the different locations (81.8%, 81.9% and 65.4% in Baltimore, Kunming and Rakai, respectively). Thus, the Euro line WB has excellent sensitivity in all regions, but poor specificity in Rakai, Uganda.
Similar to the lack of HSV-2 specificity, there are also considerable problems with specificity for the HIV Western blot in Uganda; 19 it has been hypothesized that the lack of HIV specificity could be due to cross-reactivity with HSV, malaria, other retroviruses or human leukocyte antigen antibodies. 19 While HSV-1 prevalence detected by Euroline WB between Uganda (88.4%), China (91.6%) and the USA (91.1%) is similar in this study, cross-reactivity with another virus or antibody could contribute to the decreased specificity.
To examine the best predictive testing strategy based on sensitivity and specificity as compared with the UWWB, different algorithms were analysed based on previous results from three additional assays: the Focus and Kalon ELISAs and the rapid membrane assay Biokit assay.6,8,9 When compared with the UWWB, the Euroline WB performed similarly to Kalon and Focus ELISA tests in the USA and had the highest sensitivity and specificity in China. However, no adequate algorithm using additional testing was found that increased the sensitivity and specificity of the Euroline WB to the levels seen for the Kalon and Focus assays. In summary, the Euroline WB was adequate in sensitivity and specificity for confirming HSV-2 infection for North American and Asian samples, but the assay did not perform as well as either the Kalon or Focus ELISAs in Africa.
Footnotes
Acknowledgements
This study was supported by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH). Additional support was received from the HIV Prevention Trials Network sponsored by the NIAID, National Institute on Drug Abuse, National Institute of Mental Health, and Office of AIDS Research of the NIH, Department of Health and Human Services (U01-AI-068613). The UWWB testing was supported by NIAID (P01AI030731–19). We wish to thank Charlotte Gaydos, Nancy E Maldeis and Shenghan Lai for supplying samples.