
Abstract

Sir: Prolonged survival is now a feature of patients with human immunodeficiency virus (HIV) due to the advent of highly active antiretroviral therapy (HAART) in the 1990s. 1 In the intervening years the emergence of lipodystrophy and dyslipidaemic changes in patients on such therapy became apparent, with both HIV-induced factors and iatrogenic causes having been implicated. 2 Cosmetically fat accumulation and muscle wasting can have severe psychological effects on patients, 3 while appropriate management of abnormal lipid profiles is important to prevent cardiovascular events and complications in an already debilitated patient cohort. Pravastatin 40 mg is the current accepted evidence-based treatment for such patients with lipodystrophy and dyslipidaemic changes. 4,5
As a consequence of this we carried out a retrospective study to investigate the prevalence, causes and management strategies of HIV-associated dyslipidaemia in an HIV-infected cohort in Ireland. The study was conducted with HIV patients attending Infectious Disease out-patient department clinics at St James Hospital, Dublin, Ireland, in 2005. The cross-sectional analysis of patients on lipid-lowering therapy (LLT) was performed using information retrieved from the satellite pharmacy records in the Infectious Disease Department of St James Hospital. Patients were then stratified according to dose prescribed and exposure to HAART. Specific analysis of duration of exposure to protease inhibitor (PI) therapy was performed. Lipid profiles were obtained from the patient cohort and analysed with regard to LLT prescribed.
In total, 650 patients were receiving HAART, as per satellite pharmacy records, and of those, 45 (6.95%) were receiving LLT. The mean duration of exposure to HAART in this LLT group was 76.48 months (range: 27–116), with a cumulative exposure to PI therapy ranging from 21 to 115 months (mean = 63.71).
Of these 45 patients, 40 (88.9%) were receiving pravastatin (the drug of choice in HIV patients due to its favourable metabolic pathway 6 ), with six receiving the fibrate gemfibrozil (one patient received both). The dose most used in the pravastatin group was 40 mg (60%). A comparison of all dose ranges for patients on pravastatin (with the exception of the 10 mg) shows a direct correlation between exposure time to PI therapy and statin use. Of the six patients on gemfibrozil therapy, for primary high triglyceridaemia, one patient had a triglyceride (TG) level of <3 mmol/L.
Lipid profile data were successfully obtained for 35 (77.8%) of the LLT group. Elevated TG levels were found in 21 (60%) patients, of which nine (42%) had TG levels >6 mmol/L and the highest being 6.8 mmol/L. Of the patients with elevated total cholesterol (TC) greater than 5 mmol/L, 76% (16/21) of these were between 5 and 6 mmol/L, leaving 24% (5/21) with TC levels over 6 mmol/L. Figure 1 gives a graphical representation of these variations.
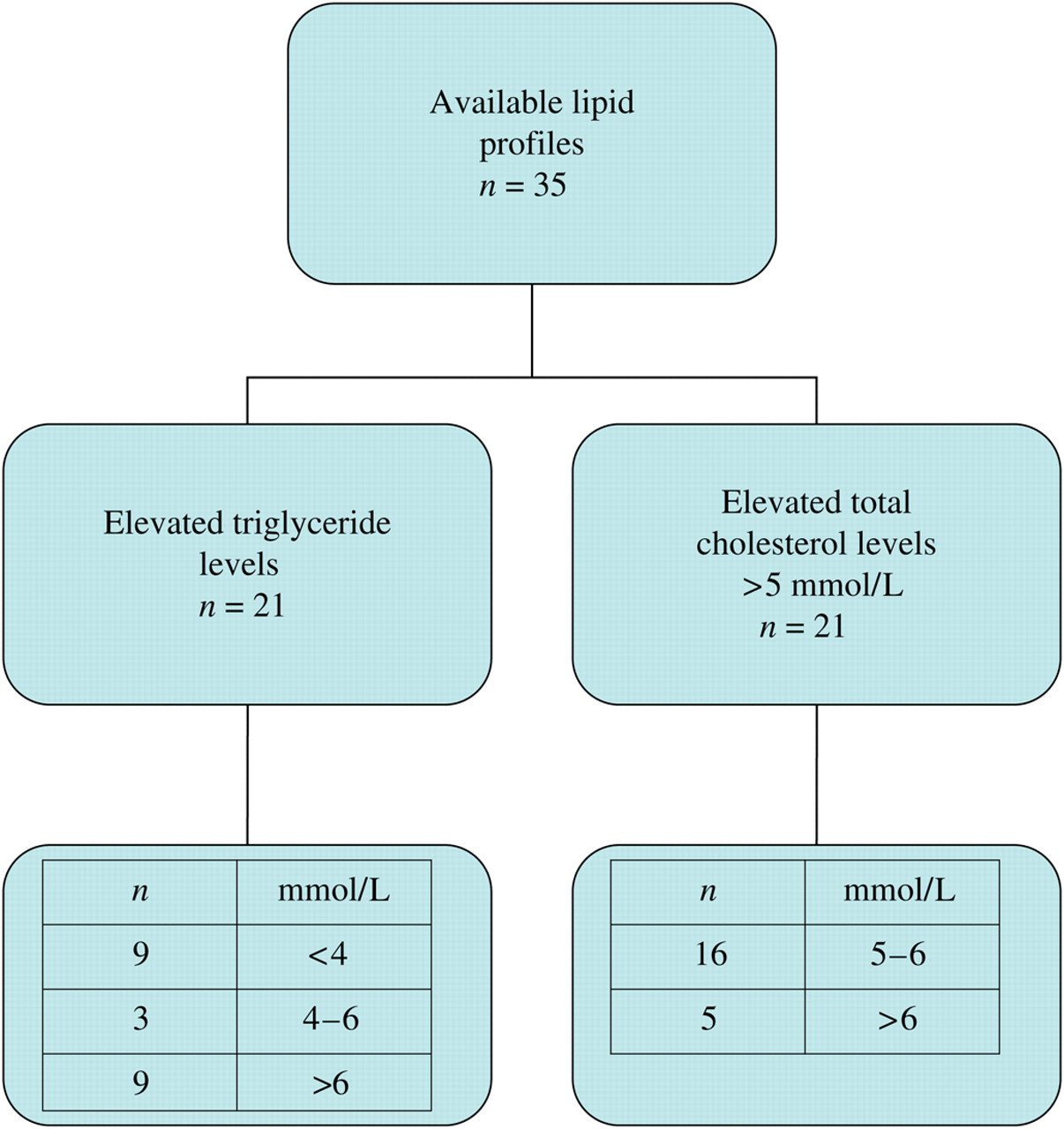
Lipid abnormalities from available patient profiles
We can conclude that there is a prevalence rate of 7% regarding lipid-lowering agent prescribing among HIV patients in this centre in Ireland. It would also appear that the management of the patients identified on LLT is not optimally controlled through the preliminary review of the lipid results, but actual reasons for this are not definitively proven. Optimal management guidelines are clearly defined and merit adherence. Ensuring that patients with altered lipid profiles are managed appropriately at this point in time will help prevent the occurrence of cardiovascular events in the future, with consequent adverse sequelae on patient morbidity, or indeed mortality and on available health care resources. Bearing in mind that this syndrome is relatively newly recognized, in tandem with the relatively recent introduction of HAART therapies, it is important that this is addressed and protocols and guidelines initiated to optimize patient outcomes with regard to management approaches.
Further studies should be undertaken in the form of a case-control study to determine the true prevalence rate and the correlation between iatrogenic exposure to PI or other agents and the development of dyslipidaemia.