
Abstract
When treating contacts of patients with sexually transmitted infections (STIs), health professionals may face conflicting ethical imperatives. We surveyed middle grade doctors in genitourinary (GU) medicine and asked how they would manage a hypothetical clinical scenario. This was analysed on the basis of principles of respect for autonomy and beneficence/non-maleficence to assess how they weigh up duties of informed consent (autonomy of patient), partner confidentiality (autonomy of partner) and the need to achieve a good medical outcome. Responses indicated that the strategies that they employ in practice –what they actually say to patients (and what they leave unsaid) – balance the conflicting requirements of these ethical principles in quite different ways, some of which appear ethically problematic.
Introduction
Most would agree that the primary goal of medicine is to benefit the patient (see Beauchamp and Childress 1 ). However, if practised without concern for the wishes of the patient, such beneficence may be regarded as paternalistic. The appropriate mechanism for reflecting such concern is usually characterized as ‘respect for autonomy’. This may be seen as setting moral limits on the professionals’ actions in pursuit of the goal of beneficence. Benefit for patients may only be achieved in ways patients would endorse through their own informed consent. The exercise of autonomy is the freedom of individuals to make meaningful choices concerning their health care ‘free from…limitations, such as inadequate understanding’ that might prevent such a choice (see Beauchamp and Childress 1 ). Concern for confidentiality also arises from the principle of respect for autonomy, allowing individuals to decide the manner and extent to which information about themselves is shared with others. 2
In sexual health clinics, we are commonly concerned with the potential exposure of our patients to infections that may be sexually transmitted. In assessing such patients, we are often aware of the infection status of any sexual partner(s). Frequently, there is a potential conflict between our beneficent desire to prevent or mitigate the effects of a sexually transmitted infection (STI) in the consulting patient together with our desire to respect his/her autonomy through enabling informed consent while also respecting the autonomy of sexual partners through protection of their confidentiality. We may, for example, respect a woman's right to make a fully informed consent and, in so doing, break the confidentiality of her sexual partner by disclosing more information than he would wish. We may respect her partner's confidentiality, but ensure that she is treated with appropriate antibiotics through coercing her consent by the limited information we provide (thus failing to respect her autonomy). Or we may respect her partner's confidentiality and be adequately respectful of her right to informed choice, but fail to produce a beneficent outcome, in that she does not receive treatment. We are in a trilemma. Can these three competing obligations be balanced – and if so how? What do doctors do in practice?
Methods
A short clinical scenario was mailed electronically to a convenience sample of mainly specialty and associate specialist doctors working in sexual health clinics in the UK.
Clinical scenario
Respondents were provided with the following clinical scenario (Box 1).
Clinical scenario
Suppose a 30-year-old nulliparous woman came in to your clinic with a ‘C4H’ contact slip (a code suggesting contact with a non-specific sexually-transmitted infection) from her regular partner of six years. He has told her he has a ‘slight bladder infection’ and that his doctor has said that she should have a check-up. She has no symptoms presently but has had occasional vulval irritation in the past. She has had no other sexual contacts since she has been with him. He saw another doctor in your clinic the previous week with a penile discharge and you can see that he had a diagnosis of non-gonococcal urethritis (NGU) with 10–20 pus cells/HPF. All his other tests are negative. You see that he has had unprotected sex with a casual female partner within the past three months.
After history, examination and appropriate tests (the only positive finding is that she has 0–5 pus cells on cervical microscopy) you suggest antibiotics ‘to be on the safe side’. She declines, saying that she does not believe in medication unless absolutely necessary, especially as they are presently trying for a baby – what do you do?
Four potential options for management were presented. Respondents were asked if they would:
Say that she has a bit of inflammation in the cervix, which requires antibiotic treatment; Say that her partner has an infection, which could be sexually transmitted and that she may be at risk if not treated with antibiotics; Say that you need to wait for her test results – wait a week until the tests for chlamydial infection and gonorrhoea come back negative. Take no further action; Say or do something else?
The scenario is intended to suggest a situation in which the male partner has a high probability of having acquired an STI with no identifiable responsible organism. He thus has a non-chlamydial non-gonococcal urethritis (NCNGU or NSU). If the scenario is followed through, her tests for chlamydia and gonorrhoea are likely to be negative. The options proposed were not chosen to represent management strategies of equal merit, but rather clinical behaviours identified in practice and highlighting contrasting solutions to the ethical problem.
Results
Fifty-nine doctors (out of 285 mailed) returned responses to the exercise. They chose options as follows (Table 1):
Options chosen by respondents
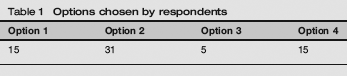
Thus, each of the options was endorsed by some respondents, while seven respondents endorsed more than one option. The option endorsed most frequently was option two – ‘ say that her partner has an infection which could be sexually transmitted…’. Most respondents elaborated in free text in support of their choice.
Themes of response
What she knows
Many emphasized the importance of establishing what she has been told by her partner and what she understands, or suspects, as a result.
Free text responses:
Ask what he has told her about the infection. Build on her reply… Explore exactly what is understood by the contact slip, what exactly they told him, whether and how he was treated, did he get a leaflet, etc. Often on probing reveals the ‘oh, yes… he did say something about NUS or something’, which I take as disclosure.
Her right to choose
I would recommend that she had treatment that day but would respect her wishes if she wanted to wait for results. I would emphasize that although this would be my recommendation based on current guidelines the decision whether to accept treatment is entirely hers to make.
Sexual ‘sharing’
I would tend to use the phrase ‘sexually shared’ rather than sexually transmitted as she could then interpret this in a way that patients often (erroneously) think sexual partners ‘share’ thrush. I would also substitute the word ‘might’ for ‘could’ as it feels more ambiguous to me… When we are intimate with people (have sex) we share our bugs with them. We have treated your partner to get rid of the bugs that were irritating him. These bugs may still be on you…we would normally offer you some treatment to get rid of those bugs so that they don't cause a problem for your partner in the future.
Procedural
Some depersonalized their advice by couching it in terms of normal procedure or policy.
I would say that since her partner had been given treatment it was our policy to treat partners together as a precaution. We always treat a couple as a single unit….
Hard-line
The (option 2) reply is a statement of fact. The male partner has put himself at risk and, consequently, his partner.
The need for confidentiality
One cannot disclose anything about him, particularly if it would lead her to suspect that he has had sex with a third party. I always explain to partners that I can't tell them what is in their partners notes and vice versa.
Non-specific urethritis (NSU) in the abstract
Sometimes I will discuss NSU in the abstract – one cause of symptoms of a bladder infection is something called NSU, have you heard of that? If someone has a contact slip I discuss with them what that code means, as I feel I can do that without breaching the confidentiality of her partner. That knowledge is in the public domain and she could find out what C4H is from another source.
Inflammation on the cervix
Despite the fact that this is medically contentious.3–6 many respondents used this as a rationale for suggesting treatment.
We have found a small amount of discharge in your cervix, sometimes this is normal and sometimes it is a sign of a sexually transmitted disease… If she is not aware of partner's treatment it becomes tricky and then I would go with [inflammation of the cervix].
Others suggested the finding of 0–5 pus cells was not pathological and not relevant. Some were emphatic…
Her cervical pus cells are normal, not a ‘positive finding’, and completely irrelevant. Option 1 is lying.
Treatment for the sake of the male partner
I…might suggest that if she is treated it would help to sort out his problem. It is sometimes uncomfortable to collude, but it is also important to ensure that the regular partner is managed effectively. I'd say that in some cases NSU is sexually transmitted and that her partner's symptoms are not likely to resolve if she doesn't have treatment.
This approach appears to place some (moral) responsibility for the health of the man on his long-term female partner, and may seem counterintuitive to some.
The greater good
My philosophy is to ensure all contacts are treated with the minimum damage to relationships while not telling lies. I am guilty of being selectively economical with the truth.
Most respondents cited her desire to start a family as an additional reason to err on the side of treatment. Those who said they would say or do something different (option 4) suggested other tactics, such as contacting the index patient to encourage further disclosure (although did not say how this would help in the consultation at hand). They also tended to adopt a ‘procedural’ approach (‘our normal practice’ or ‘we always do…’ or ‘our policy’ or ‘we treat partners automatically’). Some gave a more detailed account of the potential causes of NCNGU, but what united this group of respondents was a clear (sometimes explicit) desire to avoid the description ‘sexually transmitted’.
Discussion
While the results cannot be taken as representative of any group of doctors, they do illustrate the breadth of clinical responses that such a scenario may provoke in practice. It may be tempting to launch into the consultation in the manner recommended by the respondent providing comment M – by simply telling the patient that C4H is, of course, NSU on the basis that this information is ‘in the public domain’. (The author was able to confirm this by inserting ‘C4H’ into an Internet search engine and being able to identify ‘non-specific urethritis’ as the diagnosis within a few minutes.) Nevertheless this drives a ‘coach and horses’ through the logic of coding contact slips. Although the KC60 coding system was not designed for this purpose, it is commonly used as a vehicle to maintain confidentiality on these forms.
Sexual Health and HIV Property Type (SHHAPT) coding will doubtless be used in the same way. By implication, the use of a code conveys that the index patient has not given permission for their diagnosis to be made explicit to contacts (although this may not, in fact, be true). However, many services now ask the permission of the index patient to insert the true diagnosis in order to circumvent this uncertainty. Where the patient agrees this saves a good deal of time in assessing the level of awareness of sexual contacts, but even if NSU is written on the form, one can still not assume complete insight. Certainly, if a code is used, disclosure cannot take place on the casual basis that someone else might tell them or they might find out for themselves. Patients have a right to expect that information held about them will be held in confidence by their doctors. 8 Under General Medical Council (GMC) guidance, disclosure may be justified in the public interest if there is a ‘risk of death or serious harm’. 9 While this may apply in the passage of HIV, it is unlikely to apply in relation to a less serious STL Additionally, the harm generated by a reluctance to present to a clinic with a possible STI or pass on a contact slip may be great if confidentiality is seen to be eroded in this way. Another approach (response L) is to move directly from ‘bladder infection’ to ‘NSU’ on the basis that they may have the same symptoms. Nevertheless, a key difference would seem to be that one is sexually transmissible whereas the other is not. One might assume that once a patient attends a sexual health clinic he/she may already have an awareness of the possibility of STI. It may be that it is this implicit acknowledgment of sexual exposure allied with evident medical concern that provides the actual guarantee in practice that we have not over-stepped the mark in terms of disclosure; but again we cannot assume this insight.
If a disease can be described as ‘sexually transmitted’ this implies two things – first that it may have been sexually acquired (‘picked up’) and second that it may be sexually shared (‘passed on’ or ‘passed back and forth’). In an apparently long-term monogamous relationship, the possibility of the former is emotionally charged whereas the latter is far less so. Many respondents adopted the sexual sharing vocabulary avoiding exploration of how the infection might have been initially acquired. This may indeed be acceptable to some patients allowing for a certain amount of denial in those who might choose to adopt this as a coping strategy. It may also feel less uncomfortable to the health professional drawn into emotional identification with one or other party. Some will, however, wish to ask direct questions about the origin of the infection. At least one respondent elaborated robustly on the possibilities of acquiring a urethritis without recourse to another sexual partner:
[I] also explain that the infection could be caused by her having thrush or bacterial vaginosis, even though there's no sign of it now, him having urinary tract infection, herpes in the urethra – this is possible with monogamy – or the NSU being part of enteric Reiter's syndrome.
Lists of differential diagnoses, without discussion of the relative frequency of these diagnoses, may suggest that each explanation is as likely as the next.
This clearly depends on the circumstances, however, and an STI would seem to be the most likely diagnosis in this scenario. However, the dictum ‘first do no harm’ is often used to express the primacy of the moral obligation of non-maleficence for good reason. NCNGU may have a non-sexually transmitted cause and this must be clearly conveyed, regardless of our awareness of his other sexual partner. Were we to identify chlamydia or gonorrhoea the situation would be different, but with NCNGU we presently cannot be certain that we are dealing with an STI. In this scenario it would plainly be wrong to jeopardize the relationship by asserting otherwise.
What about sidestepping the issue by identifying an infection in her? As pointed out by many respondents, best evidence now suggests that the presence of polymorphs in the cervix has no predictive value in identifying genital tract infection in women. Any doctor aware of this fact but indicating otherwise would be perpetuating an untruth. GMC good practice guidance 10 states that good doctors are ‘honest and trustworthy’ while specific guidance to general practitioners identifies one of the roles of a doctor as a ‘health educator’. Bell, 11 in her advice to health advisers on partner notification, explicitly considers whether telling lies can ever be justified. Commonly, the act of lying may be defended on the basis that any harm is slight and ‘the end justifies the means’ (a consequentialist approach). However, consequentialism may be used to justify the breach of any moral duty unless safeguards are employed to limit its potential excesses. These safeguards are rules that cannot be broken no matter how good the outcome. Most professionals would regard the obligation of truth-telling as one such rule, and hence view any lie as a wholly unacceptable breach of trust. Option 1 thus appears ethically flawed.
Certainly, a sensitive exploration of this woman's understanding of her partner's diagnosis and the meaning of the contact slip would seem to be the wisest way to initiate any such conversation. If she fully understands his condition then the dilemma dissolves. If she reveals that her partner did mention ‘NSU’ (or something like it, as in response B), the conversation can become easier. However, if the title of the infection alone was conveyed it is still not clear that this amounted to ‘disclosure’. Her partner may not have adequately understood the pathogenesis of the condition and its possible implications, or may have simply left out important details, such as the sexual transmission of the infection.
In order to enable someone to make a medical decision that is adequately informed, the health professional must provide patients with the information that they want or need in relation to the diagnosis and appropriate treatment options. 12 In law, there are two standards of information required for a valid consent. The first is an explanation of the ‘broad nature and purpose’ 13 of the proposed treatment – something to the effect that ‘this is a prescription for an antibiotic and it is intended to treat or prevent any bacterial infection’. Such a level of disclosure would be an adequate defence against a charge of battery (unconsented touching), but a higher standard of disclosure is required to refute a charge of negligence. This standard requires that the patient should be given adequate information about the diagnosis, the treatment options and any material or significant risks that apply to each including the risks of doing nothing. 14 In order to understand the risk of doing nothing, she would have to know that her partner has a potentially sexually transmissible infection, that she may have picked it up and that medical tests might nevertheless fail to identify it in her. Such a chain of events, might eventuate from option 3. There has been no such case to date, but it is possible to imagine a scenario in which a woman in this situation sues her doctor for failing to inform her of the risk of developing pelvic inflammatory disease, even in the absence of a positive test for Chlamydia trachomatis or Neisseria gonorrhoeae. If, as a result, she did not take prophylactic antibiotics and the harm of tubal factor infertility ensued, then negligence, causation and harm would all be potentially in place for a successful action. The duty of confidentiality to her partner may be cited in defense and it may be that the public interest in maintaining his confidentiality would be judged to trump her right to informed consent. However, it serves to make the point that such an inadequately informed decision might in other circumstances be deemed unacceptable. For these reasons, option 3 also appears ethically flawed.
Conclusion
Duties of confidentiality and respect for autonomy may well conflict in trying to achieve a beneficial outcome in the management of someone exposed to an STI. Sexual health doctors recognize this as a genuine dilemma (actually trilemma) encountered not infrequently in practice. Respondents dealt with this hypothetical scenario in a number of ways: firstly trying to establish if disclosure has already occurred – if so, the dilemma dissolves. Otherwise: attempting to reduce the emotional threat of STI through subtle vocabulary change; avoiding awkward questions through presenting medical management as a routine; suggesting she should accept treatment for her partner's benefit; or dealing with STI as an abstract concept. More contentious approaches included: identifying an infection in her (on insubstantial grounds), suggesting she should accept treatment for her partner's benefit; and/or by breaking his confidence to a greater or lesser extent. Although the latter appears clearly unethical, it is not clear that any of the former approaches stands up to ethical analysis either; closing down any opportunity for exploration, providing information that is lacking in important detail, or frankly misleading, or being subtly coercive all undermine autonomy.
The best approach would seem to be a subtle exploration of insight concerning the partner's condition, along with an explanation of the way that certain infections may be sexually ‘shared’. If necessary, (on direct questioning) this might include discussion of how the infection might initially have been acquired – but, in relation to NSU, must encompass its uncertain aetiology in many circumstances. These are frequently difficult consultations, partly because we may be drawn into emotional identification. Competing obligations to absent third parties appear to have drawn many of our respondents into ethically problematic responses. We should aspire to be medically well-informed, to act as honest educators, to respect confidences and withhold judgment. The fact may be that even though there might not be a ‘perfect fit’ solution, this must not draw us into exploiting convenient falsehoods, casually breaching confidences or simply avoiding sticky conversations.
Footnotes
Acknowledgements
Thanks to Charlotte Donald for handling all electronic mailing and forwarding of responses. Also to Dr Pat Munday for comments on the text and to Drs Faryal Mahar, Sasi Rajamanaharan, Liz Broadwith and Helen Mullan for helpful input.