
Abstract
Large randomized controlled trials support the efficacy of moxifloxacin for the treatment of uncomplicated pelvic inflammatory disease (PID). This study compares the clinical outcome and tolerability of treatment with moxifloxacin 400 mg once a day or ofloxacin 400 mg plus metronidazole 400 mg both twice daily in patients diagnosed with PID. A retrospective case-notes review was performed on patients diagnosed clinically with PID before and after local guidelines were changed to recommend moxifloxacin as first-line treatment for uncomplicated PID. Before the guidelines changed, 114/134 (85%) patients received the recommended first-line therapy versus 206/257 (80%) after the change, P = 0.3. There was no difference in the clinical outcomes between the two groups; significant improvement/resolved 77% versus 70%; marginal improvement 3% versus 11%; no change/worse 20% versus 18%, P = 0.14. Moxifloxacin is confirmed to be an effective alternative to ofloxacin/metronidazole for the treatment of PID in a large urban genitourinary clinic setting.
INTRODUCTION
Pelvic inflammatory disease (PID) is an important consequence of sexually transmitted infection and is associated with long-term morbidity if not treated promptly with appropriate antibiotic therapy. Potential sequelae include impaired fertility, chronic pelvic pain and an increased risk of ectopic pregnancy. 1 Evidence-based clinical guidelines recommend that an appropriate antibiotic regimen should provide cover for Neisseria gonorrhoeae, Chlamydia trachomatis and anaerobic bacteria. 2,3 Oral ofloxacin 400 mg plus oral metronidazole 400 mg both twice daily for 14 days is recommended as an appropriate first-line therapy in both UK and USA. 2,4 This recommendation is supported by data from randomized controlled trials, which show no significant difference in cure rates between a course of oral ofloxacin and treatment with a single parenteral dose of cephalosporin followed by a course of oral doxycycline, 5,6 a regimen that has been shown to achieve similar cure rates to inpatient treatment with parenteral antibiotics for women with disease of mild to moderate severity. 7
Clinical cure rates following outpatient treatment of PID range from 70% to 100% in clinical trials, 1 but in clinical practice the results may be affected by how well patients are able to adhere to the prescribed regimen. This in turn may reflect dosing frequency and side-effect profile. In a study of compliance with oral doxycycline therapy for outpatient treatment of PID, 41% of patients stopped their medication early; 8 experiencing side-effects was one of the major reasons given for this. In a random selection of patients participating in the American PEACH study, it was reported that the prescribed two daily doses of doxycycline were taken on less than half the treatment days, and that less than 20% of doses were taken at the correct time. It was therefore suggested that there was a need to explore the effectiveness of antibiotic regimens, which are easier to take. 9
Large randomized controlled trials support the efficacy of moxifloxacin for the treatment of uncomplicated PID. 10,11 Moxifloxacin has the advantage of once daily dosing and, due to greater coverage of anaerobes than existing fluoroquinolones, does not require the addition of metronidazole.
A diagnosis of PID was made at between 4% and 6% of female attendances at a large urban genitourinary (GU) medicine clinic between 2005 and 2007. In June 2007 the local clinic policy for treatment of uncomplicated non-gonococcal PID was changed from twice daily ofloxacin plus metronidazole to once daily moxifloxacin as first-line therapy. This study compares the clinical outcome and tolerability of treatment with moxifloxacin 400 mg once a day or ofloxacin 400 mg plus metronidazole 400 mg both twice daily, in patients diagnosed with PID before and after the change in recommended first-line therapy.
METHODS
A retrospective case-notes review was performed on all patients diagnosed clinically with PID during two six-month time periods: Group 1 (1 July 2005 to 31 December 2005) when first-line treatment was ofloxacin and metronidazole, both 400 mg twice a day, and Group 2 (1 June 2007 to 31 November 2007) when moxifloxacin 400 mg once a day was the recommended first-line treatment. Cases were identified from KC60 coding data and clinic prescribing records. Patients with PID who had gonorrhoea diagnosed by cervical microscopy at their initial visit were excluded from the analysis, as the recommended treatment for this group differs from that for PID secondary to chlamydia or PID of unknown aetiology. Data were extracted from the clinical notes on patient demographics, microbiological diagnosis, therapy prescribed, follow-up rates, treatment tolerability and side-effects, treatment completion and clinical symptom improvement. Adherence to clinic guidelines for the treatment of PID and clinical outcomes were compared between the two groups. Comparisons between the two groups were analysed using χ 2 and Fisher's exact test as appropriate.
RESULTS
One hundred and thirty-four cases were available for review in Group 1 (of 152 identified) and 257 cases in Group 2 (of 272 identified). The two groups were similar with respect to age and ethnicity, and also in the proportion of patients with confirmed C. trachomatis or N. gonorrhoeae infection (Table 1). More patients in Group 1 were diagnosed with bacterial vaginosis (30.5% versus 21.4%, P = 0.048).
Comparison of group characteristics
The recommended first-line antibiotic was correctly prescribed in 114/134 (85%) in Group 1 and 206/257 (80%) in Group 2, P = 0.3. An appropriate antibiotic regimen, which was defined as any regimen providing cover for the requisite organisms, was received by more patients once the clinic policy had been changed to recommend moxifloxacin first-line (124/134 [92.5%] of Group 1 and 253/257 [98.4%] of Group 2, P = 0.004). One patient in Group 1 and two patients in Group 2 had N. gonorrhoeae identified by microscopy at their initial visit; all were correctly treated with a cephalosporin in addition to the standard antibiotic regimen. Of those who received the recommended antibiotic regimen, 63% (72/114) of Group 1 and 60% (124/206) of Group 2 attended a follow-up visit. Clinical outcome was recorded in 95% (69/72) and 92% (114/124), respectively, and divided into three categories – significant improvement/resolved; marginal improvement; and no change/worse.
The outcomes in Group 1 (ofloxacin/metronidazole) and Group 2 (moxifloxacin), respectively, were significant improvement/resolved 77% (53/69) versus 70% (80/114); marginal improvement 3% (2/69) versus 11% (13/114); and no change/worse 20% (14/69) versus 18% (21/114), P = 0.14.
In those patients who attended clinic for a follow-up appointment, it was recorded in the notes that 19% (14/72) of Group 1 reported side-effects compared with 16% (20/124) of Group 2. Most side-effects reported were gastrointestinal. However, in a greater number of cases in Group 2 (73% versus 33%) it was not recorded whether any side-effects were experienced (Figure 1).
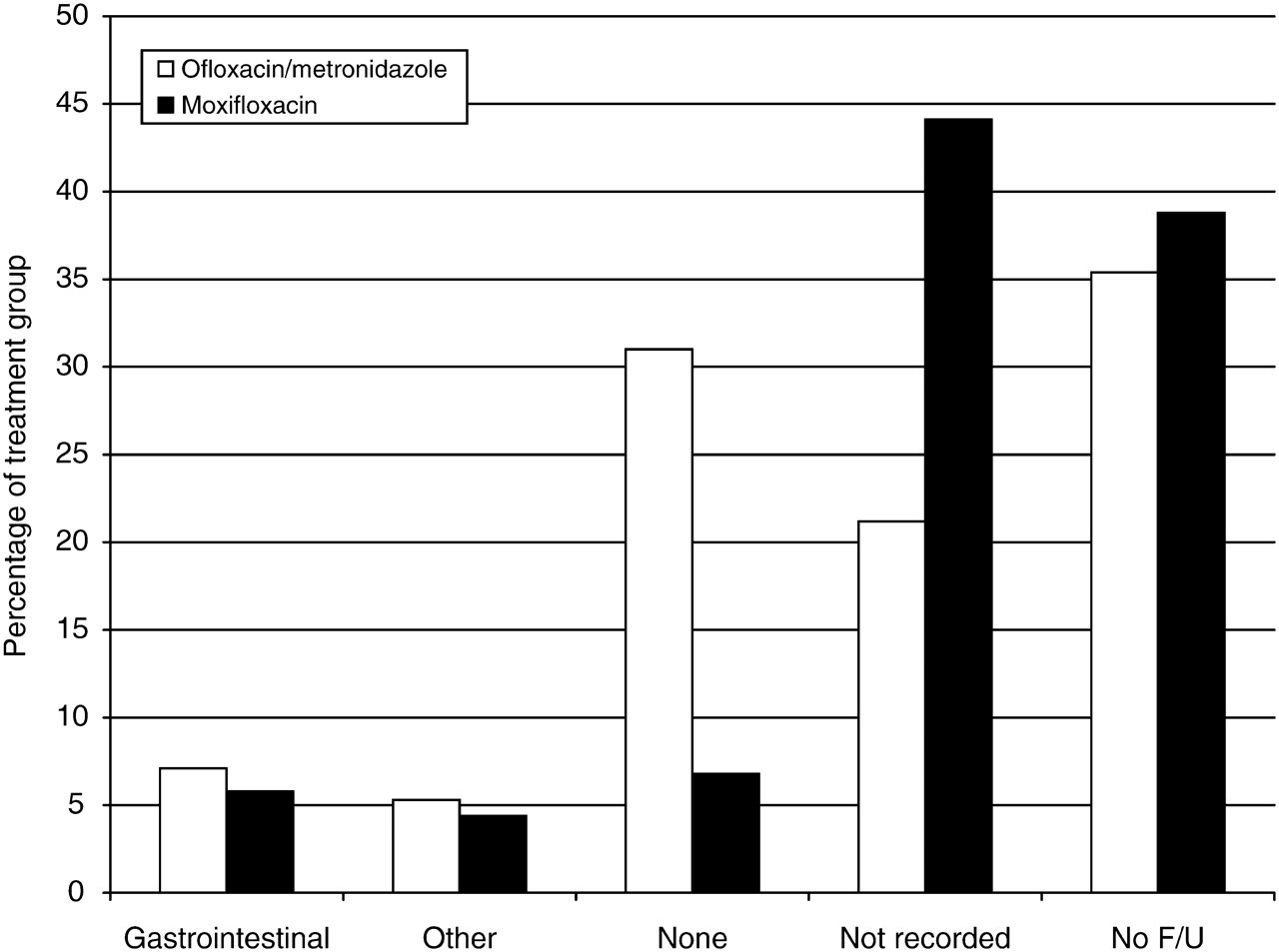
Side-effects reported by patients. No F/U = patient did not attend clinic for follow-up appointment
CONCLUSION
Clinical outcomes for patients treated for uncomplicated PID were not adversely affected by changing the recommended first-line antibiotic regimen from ofloxacin 400 mg twice daily with metronidazole 400 mg twice daily to moxifloxacin 400 mg once daily.
In addition, following the change a greater proportion of patients received an appropriate antibiotic regimen and there was a trend towards a reduction in medication-associated side-effects. The results of this study suggest that the high levels of clinical cure for moxifloxacin monotherapy in the treatment of PID reported by the MAIDEN study group are reproducible in a routine clinic setting. In addition, the response rate in this study is comparable to the 72% clinical cure rate reported in an audit of PID treatment in an urban UK GU medicine clinic using another recommended drug regimen, ceftriaxone (intramuscularly) followed by oral doxycycline and metronidazole. 12
We note an increase in the number of PID cases diagnosed between the two time periods studied. This is reflective of an increase in the number of patients attending the clinic from 2005 to 2007 and a national trend towards increased PID diagnoses. 13 There is no widely accepted flowchart in use for the diagnosis of PID; consequently, it is usual for clinical judgement to be used. Staff training and criteria for diagnosis did not change between the two study periods. The data from this observational study are therefore reflective of routine clinical practice.
This study is limited by its reliance on available information available from the case-notes for determining the clinical response and frequency of side-effects. A significant proportion did not attend for a follow-up appointment, but this did not vary between the two study periods. There was no difference between the groups with regard to the frequency of recording clinical response, but differences in the recording of side-effects and adherence to therapy make drawing firm conclusions in these areas difficult.
Moxifloxacin was initially included as one of the recommended outpatient treatment strategies in the European guidelines on management of PID updated in 2007. 3 Subsequent to the publication of these guidelines, a review of the safety of oral moxifloxacin by the European Medicines Agency has raised concerns about adverse hepatic reactions and recommended that moxifloxacin is no longer prescribed first-line in upper and lower respiratory tract infections. 14 It should be noted that this is a rare side-effect and the recommendations apply only to respiratory disease; however, in light of this moxifloxacin is no longer recommended as first-line therapy for PID in the European guidelines.
In view of these potential safety concerns, it is not appropriate to recommend moxifloxacin as first-line treatment in PID; however, it offers an effective alternative to ofloxacin/metronidazole in those unable or unwilling to take this combination.