
Abstract
The objectives of this study were to describe the findings of anal cytology screening during the first year of a unit protocol offering yearly screening to all HIV-positive men who have sex with men (MSM). Of 285 patients seen, 75% were offered anal cytology screening. Sixty-two percent of patients offered screening accepted and 21% of anal smears performed were reported as abnormal. Anal cytology screening may lead to earlier detection of anal intraepithelial neoplasia allowing for treatment before progression to cancer. This study revealed potential difficulties in follow-up of patients with high-grade precancerous disease and highlighted potential resource implications of implementing a routine screening programme.
Keywords
INTRODUCTION
Men and women with HIV infection have a much higher risk of developing anal cancer than the general population. 1 Receptive anal intercourse is a strong risk factor for anal carcinoma 2 and HIV-positive men who have sex with men (MSM) are twice as likely as HIV-negative MSM to develop anal cancer. 3 The incidence of anal cancer among MSM has continued to rise despite the introduction of combination antiretroviral therapy (cART). 4,5
Like cervical cancer, a spectrum of anal precancerous changes or anal intraepithelial neoplasia (AIN) is seen. 6 However, unlike cervical cancer there is a lack of studies of AIN to determine the progression rates of each individual stage. 7,8 There are also few data available on the outcomes of different treatment options for AIN and whether treatment of AIN prevents progression to anal carcinoma. 8 For these reasons the value of screening programmes to detect AIN remains controversial. 9
Several experts suggest consideration of anal cytology screening to detect AIN in high-risk patients. 10,11 Recently published UK guidelines do not recommend routine screening for AIN but advise that all major HIV units develop an increased awareness of anal cancer and develop guidelines for the management of suspected anal cancer and precancer. 12,13
In our unit a protocol was implemented in December 2006 to offer anal cytology screening to all HIV-positive MSM on a yearly basis. Patients with mild or moderate dyskaryosis on cytological analysis would undergo a repeat anal cytology sample six months later whereas those with high-grade dyskaryosis would be referred to the colorectal surgical team for further investigation. The purpose of this study was to describe the findings of anal cytology screening in the first year following implementation of this protocol.
METHODS
Data collection
The case-notes of all (n = 287) HIV-positive MSM attending our HIV clinic over a 12-month period after implementation of the protocol were reviewed. Data extracted were age, nationality, smoking status, nadir CD4 count, CD4 count at time of anal cytology, HIV viral load (VL) at time of cytology, any previous AIDS-defining illness, time since diagnosis of HIV, whether on cART, past history of warts and diagnosis of Chlamydia trachomatis, Neisseria gonorrhoeae, herpes simplex virus or syphilis over the previous year. Two patients were excluded from the study as they had a past history of anal cancer and were under regular surgical follow-up.
Cytology sampling
Anal cytology samples were obtained by passing a nylon sampling brush (Axibrush) 3 cm into the anal canal and gently rotating. This brush was placed in liquid-based cytology solution (Thinprep Preservcyt Solution). The material was then examined by a pathologist and graded as normal, insufficient sample, mild dyskaryosis, moderate dyskaryosis or high-grade dyskaryosis.
Statistical analysis
Data were analysed using PASW Statistics for Mac version 17.0 (SPSS Ltd, Quarry Bay, Hong Kong). Patients with insufficient samples on cytology were excluded from statistical analysis. Chi-squared tests were used for comparison of proportions and t-tests for continuous variables. Comparisons were considered significant at P < 0.05. All P values quoted are two tailed.
RESULTS
Demographics and clinical data of HIV-positive MSM attending HIV clinics during the study period (n = 285)
Figures in parenthesis represent range of values. VL = HIV viral load; ART = antiretroviral therapy; GC = Neisseria gonorrhoeae infection; HSV = herpes simplex virus infection; MSM = men who have sex with men
Of 285 patients attending clinic, 215 patients (75%) were offered anal cytology, of which 134 (62%) accepted. A total of 102 (76%) anal smears were normal and four (3%) were reported as insufficient. Of 28 (21%) reported as abnormal, 12 showed mild dyskaryosis, 15 moderate dyskaryosis and one high-grade dyskaryosis. The one patient with high-grade dyskaryosis on cytology was referred to the colorectal surgical team for examination under anaesthesia and biopsy. The passage of patients through screening is illustrated in Figure 1.
Flow diagram of anal cytology screening for HIV-positive MSM attending clinic during the study period. MSM = men who have sex with men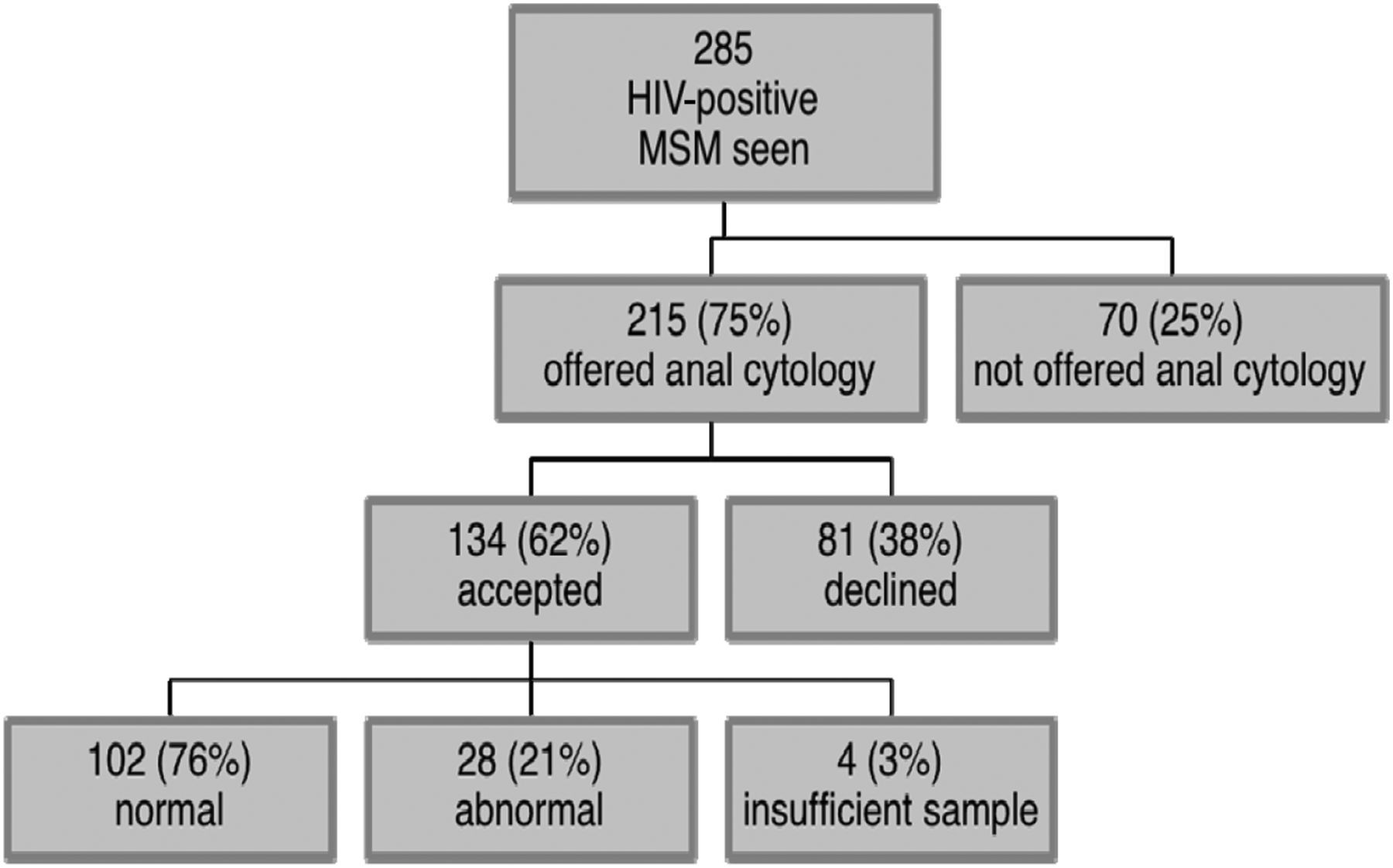
Comparison of patients with normal and abnormal cytology
VL = HIV viral load; ART = antiretroviral therapy; GC = Neisseria gonorrhoeae infection; HSV = herpes simplex virus infection
Patients not offered anal cytology screening were more recently diagnosed with HIV than those who were offered anal cytology (64 versus 81 months, P = 0.021). These patients also had higher mean nadir CD4 counts (356 cells/mm3 versus 270 cells/mm3, P = 0.002). Patients not offered anal cytology screening were less likely to be on antiretroviral therapy (58% versus 75%, P = 0.014) than those who were offered anal cytology.
Patients who declined anal cytology were less likely to have a past medical history of warts than those with abnormal anal cytology (16% versus 39%, P = 0.020) and were also less likely to have had C. trachomatis infection in the past year (8% versus 33%, P = 0.049).
DISCUSSION
Offer and uptake of screening in the first year of this programme were 75% and 62%, respectively. Both might be improved by physician and patient education and computer-assisted prompts. The proportion of abnormal anal cytologies (21%) seen in this study was lower than that reported in other studies. 4,14,15 Previous studies included a larger proportion of patients from high-risk MSM communities, patients with symptoms of anal disease or patients with previously diagnosed AIN. These patient groups would be expected to have a higher prevalence of anal cytological abnormalities than the patient population in this study.
Unlike previous studies no association was seen in this study between abnormal anal cytology and low nadir CD4 count or low CD4 count at the time of anal cytology, 16,17 possibly because the mean nadir CD4 count in both the normal and abnormal anal cytology groups was fairly high (269 cells/mm3 and 317 cells/mm3, respectively). However, patients with abnormal anal cytology were significantly less likely to be on antiretroviral therapy than those with normal anal cytology (P = 0.002). Patients with abnormal anal cytology were more likely to have had C. trachomatis infection within the year preceding anal cytology (P = 0.049). This may be a marker of high-risk sexual behaviour and an increased likelihood of anogenital HPV infection.
Patients not offered anal cytology screening had a shorter period of time from HIV diagnosis than those who were offered anal cytology (P = 0.021). These patients also had higher nadir CD4 counts (P = 0.002) and were less likely to be on antiretroviral therapy (P = 0.014) than those who were offered anal cytology. This suggests that a limiting factor in offering anal cytology screening may be time constraints in clinic, particularly following a recent HIV diagnosis. Patients who declined anal cytology were less likely to have a past medical history of genital warts (P = 0.049) and were also less likely to have had C. trachomatis infection in the past year than those with abnormal anal cytology (P = 0.020). This group may engage in lower risk sexual behaviour and possibly consider themselves to be at lower risk of anal cancer than those accepting anal cytology screening. It may also be that patients were more likely to accept anal cytology screening when offered at the time of a routine STI screen, so those declining STI screening did not have anal cytology performed. Continued education is needed to increase general awareness of anal cancer in HIV-positive MSM.
Further investigation of patients with abnormal smears by anoscopy as recommended by many experts 18,19 is not possible in our unit due to a lack of trained personnel. All patients found to have high-grade dyskaryosis are therefore referred to the colorectal surgical team at a local hospital for visualization of the anal mucosa and consideration of biopsy. Our inability to provide comprehensive follow-up and the findings of others who have reviewed similar screening programmes 9,16 suggest that routine annual screening may not be the best use of resources, as well as generating unnecessary anxiety.
Anal cytology sampling is a straightforward procedure and implementation of an anal cytology screening programme may lead to earlier detection of high-grade AIN allowing treatment before progression to anal carcinoma. 18,19 However, an increased awareness of the risk anal carcinoma among HIV-positive patients and HIV physicians together with regular examination of those with high-grade dyskaryosis at baseline may prove to be the most cost-effective approach.