
Abstract
We present a case of Bacille Calmette-Guerin (BCG) lymphadenitis following immunization of a health-care worker with risk factors for HIV but undiagnosed infection. This case highlights the potential risks of BCG and clearly demonstrates the need to consider HIV testing in all patients prior to BCG vaccination.
Introduction
Bacille Calmette-Guerin (BCG) is contraindicated in HIV-infected individuals 1 in view of the recognized risk of local and disseminated disease.2,3 Although BCG is currently targeted at infants within high-risk groups in the UK, a significant number of adults continue to receive it, including health-care professionals and contacts of active Mycobacterium tuberculosis infection. As some of these individuals remain unaware of their HIV status, there is the potential to cause iatrogenic BCG disease.
We describe a case of BCG disease in a health-care worker with previously unrecognized HIV.
Case Report
A health-care worker from sub-Saharan Africa presented with axillary lymphadenopathy at 14 weeks of pregnancy. An antibody test confirmed HIV-1 infection. CD4 count was 64 cells/μL and viral load 48,985 copies/mL; examination and baseline investigations were otherwise unremarkable. A fine needle aspirate grew Mycobacterium bovis, BCG strain. She received the BCG vaccine following a negative tuberculin skin test during an occupational health assessment three months earlier. She had no other recollection of BCG vaccination but three characteristic scars were visible over the left deltoid, suggesting previous immunization.
Co-trimoxazole was initiated followed by rifampicin, isoniazid and ethambutol. A week later, antiretroviral therapy was started with zidovudine, lamivudine and nevirapine. The lymphadenopathy resolved within a month. Her CD4 count increased to 309 cells/μL and viral load became undetectable by week 24. She completed nine months of antituberculous therapy without complications and delivered a healthy child, who remains HIV-negative.
Discussion
The revised paediatric classification system 2 outlines four categories of BCG complications: local, limited to the inoculation site; regional, affecting the lymph nodes; distant, involving a separate site such as the lung; and disseminated, infection at two or more distant sites or positive blood/bone marrow cultures. The latter three are classified as BCG immune reconstitution inflammatory syndrome if occurring within three months of initiating antiretroviral therapy.
In the absence of HIV, BCG complications are rare and mainly associated with cellular immunodeficiency. 2 However, it has been estimated that HIV-positive infants have a several 100-fold increased risk of disseminated BCG disease, irrespective of the presence of HIV symptoms. 3
Whether HIV-infected adults are at increased risk of disseminated disease following BCG vaccination is more controversial. Only a few cases have been reported in the literature,4–13 most with either local or regional disease; see Table 1. The interval between inoculation and complications can be up to 30 years. Although M. bovis is inherently resistant to pyrazinamide, 6–9 months of chemotherapy with at least two other antituberculous drugs appears to be effective.4–13 There is a high mortality in HIV infected children with distant or disseminated BCG disease, 2 but the prognosis in HIV infected adults appears more favourable.4–13
Summary of clinical data on ten published cases of BCG disease in HIV-positive adults
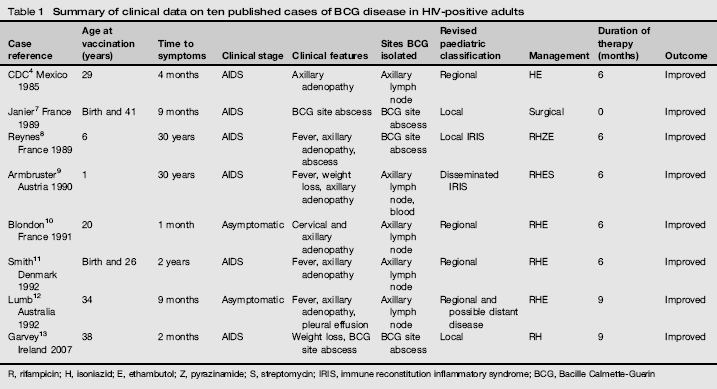
R, rifampicin; H, isoniazid; E, ethambutol; Z, pyrazinamide; S, streptomycin; IRIS, immune reconstitution inflammatory syndrome; BCG, Bacille Calmette-Guerin
With the recent influx of health-care professionals to the UK from areas where HIV is prevalent, there is a significant risk of undiagnosed HIV in this group. HIV testing prior to BCG immunization is therefore highly pertinent; all the more so in view of the higher prevalence of skin anergy in the HIV-positive population. 14 A recent study has shown that offering HIV testing in this setting is well accepted. 15
Ideally an assessment of the cost-effectiveness of routine HIV testing prior to BCG vaccination should be performed. Given that most cases of BCG disease probably occur in resource-limited settings, and remain unreported, this may be challenging and any calculations may underestimate the cost-effectiveness of this strategy. The authors feel that HIV testing should be recommended prior to BCG vaccination in adults. This should be included in the UK national guidelines for HIV testing 16 and highlighted to occupational health professionals and others offering BCG vaccination.