
Abstract
Giant cell hepatitis (GCH) has been rarely described in adult HIV patients, and its outcome remain unknown. We report two cases of GCH among 81 HIV patients co-infected with the hepatitis C virus (HCV). Both patients had a sustained virological response, suppression of HCV viral load and HIV viral suppression after highly active antiretroviral therapy. Our findings would suggest that the presence of giant cells does not influence the clinical course of hepatitis.
Introduction
Giant cell hepatitis (GCH) is a rare form of hepatitis reported in different settings such as autoimmune disorders1,2 and liver transplantation3,4 and generally has a poor prognosis.
Multinucleated giant cells have been also reported among the histopathological findings in the liver of HIV/hepatitis C virus (HCV) co-infected patients.5–8 Despite full clinical and histological evaluations, it is still debatable as to whether giant cell transformation should be considered a specific disease process, clinically associated to severe course. Here we report two cases of GCH in HIV/HCV-infected individuals with favourable outcome.
Case Report
Patient 1 was a 41-year-old man diagnosed with HIV and Hepatitis C in 2000. Highly active antiretroviral therapy (HAART) with emtricitabine, tenofovir and lopinavir/ritonavir was introduced for low CD4+ cell count (227 × 106/L), in 2008. Viral suppression (HIV RNA below 50 copies/mL) was achieved with an increase of CD4+ cells (774 × 106/L). HCV RNA level was 2.634.737 IU/mL (TaqMan HCV; Roche Molecular Systems Ine, Branchburg, NJ, USA) with genotype 1 and alanine aminotransaminase (ALT) level was 72 (Table 1). After liver biopsy he was treated with 180 μxg pegylated alpha-interferon weekly and 1200 mg/day ribavirin. Four weeks after treatment, the HCV-RNA level (below 15 IU/mL) and HIV-RNA remained undetectable. At six months under treatment the HCV-RNA level is undetectable and liver functional tests are normal.
Clinical findings in biopsies with giant cell change

HCV, hepatitis C virus
HCV and HIV loads are indicated as log 10 IU/mL and log 10 copies/mL, respectively
Patient 2 was a 47-year-old man diagnosed with hepatitis C infection in 1998 and with HIV infection in 1999. HAART regimen with lamivudine, tenofovir and lopinavir/ritonavir was started for low CD4+ cell count (208 × 106/L) and HIV viral load of 112.120 copies/mL. Thereafter, viral suppression (HIV-RNA below 50 copies/mL) was achieved with an increase of CD4+ cells (404 × 106/L). The HCV-RNA level was 3.545 IU/mL with genotype 3a and his serum ALT level was 55 (Table 1). Combined treatment with 180 μg pegylated alpha-interferon weekly plus 1000 mg/day ribavirin was introduced. Four weeks later, the HCV RNA level became undetectable (below 15 IU/mL), with normal ALT level. HIV-RNA remained undetectable. At six months after the end of therapy, a sustained viral response is achieved.
In both patients liver biopsies showed findings typical of chronic hepatitis C (Table 2), with several syncytial giant hepatocytes in pericentral liver biopsy (Figure 1). Mild macrovacuolar liver steatosis was observed in patient 2. In patient 1 histological activity index was 9; fibrosis grade 4/6 according to Ishak et al 9 . In patient 2 histological activity index was 6; fibrosis grade 3/6. No other histological changes were found in the biopsy specimens to suggest pattern of injury from drug effect. Both immunohistochemical technique on the biopsy sample for herpes simplex virus (HSV), Epstein-Barr virus (EBV), human herpes virus 8 (HHV-8) and cytomegalo virus (CMV) and polymerase chain reaction assays for viruses B, CMV, EBV, HSV-1, HSV-2, varicella zoster virus, parvovirus B19, HHV-7 and HHV-8, adenovirus and paramyxovirus were negative (Figure 1).
Histological findings

HAI, histological activity index
HAI and fibrosis score sec. Ishak et al. 1995
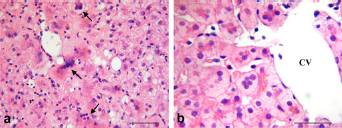
Representative images of haematoxylin-eosin-stained liver sections, (a) Several syncytial giant hepatocytes (arrows) are present in pericentral areas of liver biopsy specimen; (b) High power of giant multinucleated hepatocytes is present near the centrilobular vein (CV) displaying multiple nuclei and glassy cytoplasmic change. Bars: = 50 μm
Discussion
Adult GCH is not a frequent pattern of liver injury and is commonly associated with autoimmune hepatitis type I and II2,10 or viral infection.11–13 More recently it has been described in chronic hepatitis C8 and in active HHV-6 infection, especially in liver transplantation recipients.3,4
The information about the outcome of HIV-HCV co-infected patients associated with the presence of GCH is lacking and the presence of giant hepatocytes may be non-specific finding. 14 Moreno et al. 6 have described two cases of GCH among 243 HIV/HCV co-infected patients, with unfavourable outcome in one patient. More recently, Micchelli et al? described 22 cases (18 individuals) of GCH without aggressive course. We observed two cases of GCH out of 81 HIV/HCV co-infected individuals, with a prevalence of 2.4%. The clinical outcome of hepatitis in our cases was favourable, probably due to the successful treatment with pegylated alpha-interferon plus ribavirin and HAART; both showed suppression of HCV and HIV viral load. The giant cell changes were patchy and were found exclusively in zone 3 hepatocytes as previously noted. 15 Pathogenesis of liver damage in patients with HIV and HCV co-infection is complex and multifactorial.16,17 There are two possible mechanisms for giant cell transformation: nuclear division without cytoplasmic division, and fusion of individual cells to form a syncytium. 2 Hepatic giant cell transformation can be directly related to HIV virus, as observed in other organ tissues where it induces cell fusion. 18 No strong association with any specific drug, although a drug effect remains an important possibility.
Our observations suggest that in HIV/HCV setting, giant cell transformation of hepatocytes, when not extensive, should be considered as a random event, which does not lead to harmful clinical course of hepatitis, probably representing a regenerative response of hepatocytes.