
Abstract
Summary
The aim of the study was to evaluate the sensitivity of patients’ self-sampled vaginal specimens, first-catch urine (FCU), combined vaginal/FCU specimens and endocervical specimens for detecting chlamydial infection in women. Women attending sexually transmitted disease clinics, youth clinics and a women's health clinic were enrolled. They self-collected a vaginal specimen with two swabs, which were placed into a sterile tube and into a tube containing a buffer medium, respectively. An FCU sample was collected and aliquoted into both an empty tube and the tube containing the vaginal swab. A clinician collected an endocervical swab. The samples were sent to laboratories for analysis using polymerase chain reaction testing and strand displacement amplification testing, respectively. The sensitivities calculated in all 171 Chlamydia trachomatis-infected women were equal for endocervical specimens (97.1 %), vaginal specimens (96.5%) and combined vaginal/FCU specimens (95.3%), whereas the sensitivity for FCU was significantly lower (87.7%). The sensitivity of vaginal specimens for the detection of C. trachomatis is as high as that of combined vaginal/FCU specimens.
Introduction
Chlamydia trachomatis is the most common cause of bacterial sexually transmitted infection (STI) worldwide. 1 The genital infection is mostly asymptomatic, especially in women. 2 Opportunistic screening programmes were introduced in the 1980s and most chlamydial infection diagnosed in Swedish women is still found by this intervention despite the legislation passed in 1988, which included mandatory partner notification. 3 The introduction of nucleic acid amplification tests (NAATs) for diagnosis was a major step forward, enabling more feasible sampling, and first-catch urine (FCU) is at present the sample of choice in men. Several studies, however, have indicated that FCU as the sole specimen in women may not have satisfactory sensitivity. 4 6 Self-sampled vaginal swabs have in recent years been proven to be an appropriate specimen with sensitivity comparable with endocervical specimens.4,7
As a means of reducing costs, endocervical swabs placed into the FCU sample, compared with the same specimens sampled and analysed separately, did not show any significant difference in sensitivity in a Swedish study. 8 Most chlamydial infections in women are asymptomatic and it can be assumed that a request for gynaecological examination might make some women abstain from testing. Many women's clinics, women's health clinics and youth clinics do not have facilities to make FCU testing feasible, such as nearby toilets. Vaginal sampling may be performed more easily, since only privacy is needed. If a combination of FCU and self-sampled vaginal specimens (analysed as one sample as a means for reducing costs) could be shown to have a higher sensitivity compared with separate FCU or self-sampled vaginal specimens, patients might be prepared to perform this procedure. Only one study has, to our knowledge, been published where combined self-sampled vaginal specimens and FCU have been compared with endocervical specimens or the separate vaginal or FCU specimens per se. 9 This study showed a higher sensitivity for the combined specimens. 9 In at least four counties in Sweden (2009) the combined FCU/vaginal swab specimen has been introduced as the recommended sampling method (personal communication).
The aim of the current study was to evaluate the sensitivity of patients’ self-sampled vaginal specimens, FCU, combined vaginal and FCU specimens and endocervical specimens in the detection of genital chlamydial infection in asymptomatic women.
Methods
Study population
Patients
The study was approved by the regional research ethical committee of Linköping. Initially, starting in October 2006, women were enrolled due to partners’ chlamydial infections when they attended the outpatient sexually transmitted disease (STD) clinics at Linköping University Hospital, Linköping and Ryhov County Hospital, Jönköping. In addition, from April 2007, the youth clinics in Linköping and Jönköping as well as the women's health clinic in Linköping recruited patients. At the women's health clinic most of the women enrolled already had a confirmed positive C. trachomatis test sampled from the endocervix in a screening context. They were enrolled for new sampling at the time of starting antibiotic treatment. In October 2007, patients were also included at the STD clinic in Norrköping. Recruitment was concluded in January 2009. Data were collected in all centres on a detailed standardized questionnaire regarding: the reasons for attendance; age; symptoms (vaginal discharge, urethral pain during micturition, intermenstrual or postcoital bleeding and lower abdominal pain); previous chlamydial infections; date of last chlamydial testing; and date of last unprotected sexual intercourse and antibiotic usage (type and indication for treatment) during the last three months.
Sampling
Patients
All patients were asked not to micturate within one, preferably two, hours before sampling. Informed consent was obtained by a nurse or a midwife, who also gave the patient oral and written information about the sampling procedure. In 92.5% (290/317) of the cases the patients’ self-samp ling was performed prior to the gynaecological examination and the endocervical sampling. Patients were instructed to insert two swabs 3–4 cm into the vagina and rotate them firmly three times. The participants were instructed to micturate the first 30 mL, at most, of FCU into a plastic cup, without previously having cleaned the area. The FCU was poured (maximum of 10 mL) into each of two polypropylene tubes (Sarstedt, Nümbrecht, Germany). The vaginal swabs were placed into the Sarstedt's tubes, one in each, containing a 2-SP medium or Becton Dickinson (BD) CT/GC swab sample diluent. During the subsequent examination, a physician, an experienced nurse or midwife, depending on which clinic the patient had attended, used a swab for endocervical sampling. The physicians also sampled endocervical, urethral smears and vaginal wet smear for microscopic examination.
At the clinics in Linköping and Norrköping, Polyacrylamide swabs (Copan, Brescia, Italy) were used for vaginal and endocervical sampling. The four samples (i.e. vaginal, endocervical, FCU and a vaginal swab in FCU) were sent the same day by ordinary mail (ambient temperature) to the Department of Laboratory Medicine, Microbiology Section, örebro University Hospital, örebro. At the clinics in Jönköping, BD ProbeTec ET CT/GC swabs (Becton Dickinson, Franklin Lakes, NJ, USA) were used for vaginal and endocervical sampling. The four different samples for each patient were sent the same day (ambient temperature) to the Department of Clinical Microbiology, Ryhov County Hospital in Jönköping.
Microbiological analysis
At the Department of Laboratory Medicine, Microbiology Section, örebro University Hospital, DNA extractions of the samples were performed immediately on arrival using the MagNa®PureLC (Roche Molecular Corporation, Indianapolis, IN, USA). All samples were in the first period of the study tested using the COBAS Amplicor Chlamydia trachomatis Test® (Roche Diagnostic Systems Inc., Branchburg, NJ, USA) as described by the manufacturer. Due to the new variant of C. trachomatis discovered in Sweden by Ripa and Nilsson, 10 from 1 March 2007 the diagnostic test system was changed to the LightMix 480HT polymerase chain reaction (PCR) (TIB MOLBIOL GmbH, Berlin, Germany) on a LightCycler 480 (Roche Diagnostic Systems) as described previously. 11 From 13 August 2008, a CTM CT v2.0 (Roche Molecular Systems, Branchburg, NJ, USA) on a COBAS Taqman48 Analyser (Roche Molecular Systems) was used as described by the manufacturer. 2
At the Department of Clinical Microbiology, Ryhov County Hospital in Jönköping, DNA extractions were performed immediately on arrival of specimens by using BD Probetec™ ET Lysing Heater (strand displacement amplification [SDA] assay; Becton Dickinson). The specimens were tested by a BD ProbeTec™ ET DNA SDA assay (Becton Dickinson) according to the manufacturer's instructions.
All samples from each patient were tested using one and the same NAAT diagnostic system. In both laboratories all samples were tested for the detection of inhibition. Every positive test specimen was re-tested from the original specimen (DNA extracts) using the original diagnostic test system. A repeat positive test of a specimen was stated as a true positive. Sensitivity was measured by a true positive test by any sampling method as the denominator and the true positive by sample method as the numerator.
Statistical analyses
Exact binomial confidence intervals for the sensitivity were calculated and exact binomial tests were performed for the discordant outcomes. Fisher's exact test was used to test differences in proportions (SPSS version 17.0, IBM, Chicago, Illinois, USA).
Results
A positive chlamydia test was found in 172 of the 318 enrolled women. In one woman, endocervical sampling was not performed and hence she was excluded from the analysis. The remaining 171 women had a median age of 21 years (range 14–38). Of those, 99, 36 and 36 women were diagnosed at the STD clinics, women's health clinic and youth clinics, respectively. There was no significant difference in the rate of discordant tests (i.e. having both negative and positive chlamydial sampling sites) between the 113 asymptomatic C. trachomatis-infected women (n = 19, 16.8%) and the 58 infected women with symptoms of infection (n = 7, 12.1%) (P = 0.50).
Outcome of Chlamydia trachomatis tests from different specimens and NAATs in Chlamydia trachomatis-positive women (n = 171) and in subpopulations
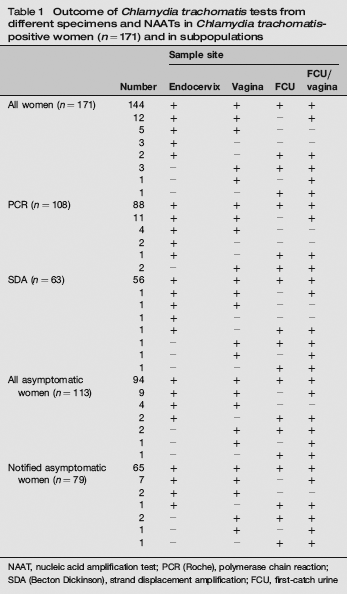
NAAT, nucleic acid amplification test; PCR (Roche), polymerase chain reaction; SDA (Becton Dickinson), strand displacement amplification; FCU, first-catch urine
In the 113 asymptomatic women, the sensitivities for endocervical, vaginal, combined vaginal/FCU and FCU specimens were 96.5% (91.2–99.0%), 97.3% (92.4–99.5%), 96.5% (91.2–99.0%) and 87.6% (80.1–93.1%), respectively. In the comparison of discordance of FCU versus each of the other specimens no significance was found (P = 0.15, 0.63 and 0.18, respectively).
Among the 21 of 26 women with a discordant result from sampling and a negative FCU, 13 had a bladder incubation time of more than two hours and a further seven more than one hour. Incubation time was not noted in the protocol from one patient. However, only one of the remaining six women with discordant results, but with a positive FCU, had an incubation time of more than two hours.
When the C. trachomatis-positive women who performed self-sampling after, and not before, the gynaecological examination (n = 15) were excluded in the comparison, the sensitivity for endocervical, vaginal, combined vaginal/FCU and FCU specimens were as follows: 97.4% (152/156, 95% CI 93.6–99.3), 97.4% (152/156, 95% CI 93.6–99.3), 95.5% (149/156, 95% CI 91.0–98.2) and 87.2% (136/156, 95% CI 80.9–92.0), respectively. Thus, FCU had a significantly lower sensitivity compared with all but the combination vaginal/FCU sampling. When, however, the discordant outcome for specimens of FCU and vaginal/FCU were compared (n = 13), the FCU was significantly less sensitive (P = 0.0024).
Outcome of Chlamydia trachomatis tests from different specimens and polymerase chain reactions in C. trachomatis-positive women (n = 108)
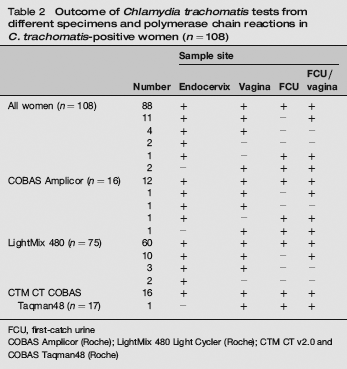
FCU, first-catch urine
COBAS Amplicor (Roche); LightMix 480 Light Cycler (Roche); CTM CT v2.0 and COBAS Taqman48 (Roche)
Discussion
Patient-collected vaginal sampling has, ever since the first published report in 2003 and in several studies thereafter, been shown to be sensitive and convenient.4,9,13
Theoretically, the combination of vaginal swabs with FCU could increase sensitivity, compared with each specimen alone, as has been demonstrated for the combination of endocervical swabs and FCU in C. trachomatis-infected and Mycoplasma genitalium-infected women.8,14 There is, however, limited previous knowledge as to whether combined vaginal and FCU specimens yield a similar beneficial outcome. To our knowledge there is only one published study to date, the outcome of which supported the hypothesis. 9 The present study confirms previous studies9,15 that the addition of FCU and vaginal specimens analysed separately detects more C. trachomatis-infected women than do the combination of FCU/vaginal specimens sampled and analysed as one specimen. A higher bacterial load could be assumed to exist and cause a higher degree of inflammation in symptomatic women, with less discordant test results from sampling sites as a consequence, compared with those women without symptoms. We could not, however, detect any significant difference in sensitivity between asymptomatic and symptomatic women.
Five women had a C. trachomatis-negative FCU and negative combined vaginal/FCU sampling as well, but C. trachomatis-positive vaginal specimens. Urine is known to contain inhibitors for NAAT assays, which may be the reason for decreasing the NAAT testing sensitivity, when the vaginal swab is transported in the urine-containing tube.
Two different NAATs were used in the study, but only one method per patient. The number of C. trachomatis-positive women with any negative sampling site was considerably lower when tested by the SDA assay, but we have no reason to believe that there exists any important difference in sensitivity between SDA and PCR, since no inhibitions or negative test results of initially chlamydial-positive samples were seen at the re-runs. Other studies either confirmed this conclusion or showed no disadvantage of PCR compared with SDA, when FCU, vaginal sampling and endocervical sampling were studied.4,16
A minority of patients (8.5%, 27/317) in the present study did their self-sampled testing after the gynaecological examination and the endocervical sampling.
Physicians’ endocervical sampling, gynaecological examination and, in many cases, sampling of smears for microscopic examination were performed before patients’ self-sampling. This could be a disadvantage for self-sampling specimens when comparing different specimens, since the highest bacterial load could be assumed to exist in the endocervix. However, no such disadvantage could be found in the 15 C. trachomatis-positive women, of whom 12 were positive in all specimens. Since the introduction of NAATs, problems of interpretation have arisen, especially with regard to specificity since the use of ‘gold standard’ was tissue culture, which is a less sensitive method.17,18 A weakness of the present study could be the use of only one NAAT diagnostic method, which was re-run for confirmation. To determine the accuracy of a NAAT result at least two NAATs should give the same test result.17,18 The aim of the present study, however, was not to study the efficacy of the NAATs, but different sampling sites and procedures. Since a repeat positive test from the initial specimen was required to define a true positive as well as inhibition control tests, we believe our results are valid. Nevertheless, the conclusions drawn from these results only apply to the two NAATs used in the study. These NAATs are in fact those that were in use in Sweden during the study period.
In many clinics there are limited facilities for FCU testing because of a lack of accessible toilets. This was, in fact, one reason for limited enrolment at one of the youth clinics participating in the study. Vaginal sampling is in this sense more feasible and convenient. There is evidence that women prefer FCU or vaginal sampling if gynaecological examination is not needed for other reasons.9,13,19,20
Vaginal sampling may have limited application during menstrual periods. This aspect was not a primary aim of the present study, but at one STD clinic eight of 86 enrolled women were documented to be menstruating. One of the three C. trachomatis-positive menstruating women had negative vaginal, FCU and combined specimen tests.
Although all women were instructed in writing and orally to void a maximum of 30 mL, it cannot be excluded that misunderstandings arose. On the other hand, this would happen in a ‘real’ setting too. The primary recruitment criterion of the study was partners’ confirmed or alleged chlamydial infection and almost half of those patients enrolled (48.3%, 116/240) had a C. trachomatis infection detected, which indicates the importance of partner notification. This finding is in accordance with previous studies.2,21
In conclusion, vaginal sampling for detecting C. trachomatis infection in women is a reliable and convenient method. The present study showed self-collected vaginal sampling to be as sensitive a method as clinician-collected endocervical sampling and combined FCU/vaginal sampling. The combination of vaginal specimens and FCU did not add any further advantage.
Footnotes
Acknowledgements
We are most grateful to the staff at the STD clinics in Jönköping, Linköping and Norrköping (especially to Ann-Louise Gross, Tordis Larsson, Margreth Wastesson and Jeanette Groenheit) and also to the staff at the youth clinics in Linköping and Jönköping as well as the women's health clinic in Linköping (especially to Pia Cederholm). We also thank Jonas Swanberg, Department of Clinical Microbiology, Ryhov County Hospital in Jönköping for information about the laboratory testing procedure of specimens sampled in Jönköping. We are also most grateful to Lars Valter for statistical computations.
This work was funded by the Medical Research Council of Southeast Sweden, ALF grants from the County Council of östergötland and by the Department of Communicable Disease Control, County of östergötland.