
Abstract
A 47-year-old man presented to his general practitioner (GP) with painful swelling of his right testis. He was diagnosed with epididymo-orchitis and a two-week course of erythromycin 500 mg four times daily was prescribed by his GP. Despite initial improvement, his symptoms persisted and he was referred to the local urology department. His sexual history revealed one lifetime sexual contact. A midstream urine sample grew non-lactose fermenting coliforms sensitive to ciprofloxacin and a two-week course of ciprofloxacin 500 mg two times daily was prescribed. Despite clinical improvement, a persistent suspicious abnormality on the ultrasound scan of his right testis prompted a right radical inguinal orchidectomy to exclude malignancy. Further diagnostic tests including histopathology excluded malignancy but confirmed tertiary syphilis. A comprehensive literature search revealed only 11 confirmed cases in the past 59 years.
INTRODUCTION
There are many causes for testicular swelling including benign conditions, malignancy and infection. The majority of these cases are regarded as straightforward to investigate, diagnose and manage. However, we were recently presented with a very rare case of testicular swelling. After extensive investigation the cause was identified as tertiary syphilis presenting as orchitis. A comprehensive literature search revealed only 11 confirmed cases in the past 59 years. The case was presented at the Royal Society of Medicine's Urology Section annual clinico-pathology meeting this year and stimulated much interest and debate. The case highlights potential lessons for practitioners and may influence their current practice, as syphilis in all its forms is on the rise.
CASE REPORT
A 47-year-old Indian man presented to his general practitioner with a painful right testicular swelling. Epididymo-orchitis was diagnosed and two weeks of erythromycin (500 mg four times daily) prescribed. Despite initial improvement, symptoms persisted and he was referred to Ealing Hospital Urology Department. Review revealed no urinary symptoms or past medical history of note and he took no medication. He had married in the UK in his teens and divorced eight years ago; his wife was his only sexual partner. He denied intravenous drug use. Examination revealed a tender right testicular swelling, with a thickened epididymis. A midstream urine sample grew non-lactose fermenting coliforms sensitive to ciprofloxacin. Blood tests revealed a white cell count of 11.9 × 109/dL (3–10 × 109/dL) and a C-reactive protein of 76 mg/L (<5 mg/L). A two-week course of ciprofloxacin (500 mg two times daily) was prescribed.
Further tests included an ultrasound (USS) of his testes and an unremarkable flexible cystoscopy. Ultrasound demonstrated an enlarged right testis (5.3 cm × 3.5 cm × 4.9 cm), with three segmented necrotic cystic areas and increased peripheral vascularity (Figure 1), suggesting tuberculous/bacterial abscesses, cysts or malignancy. Microscopy and culture of three early morning urine samples were negative for Mycobacterium tuberculosis. Tumour markers were within normal limits.
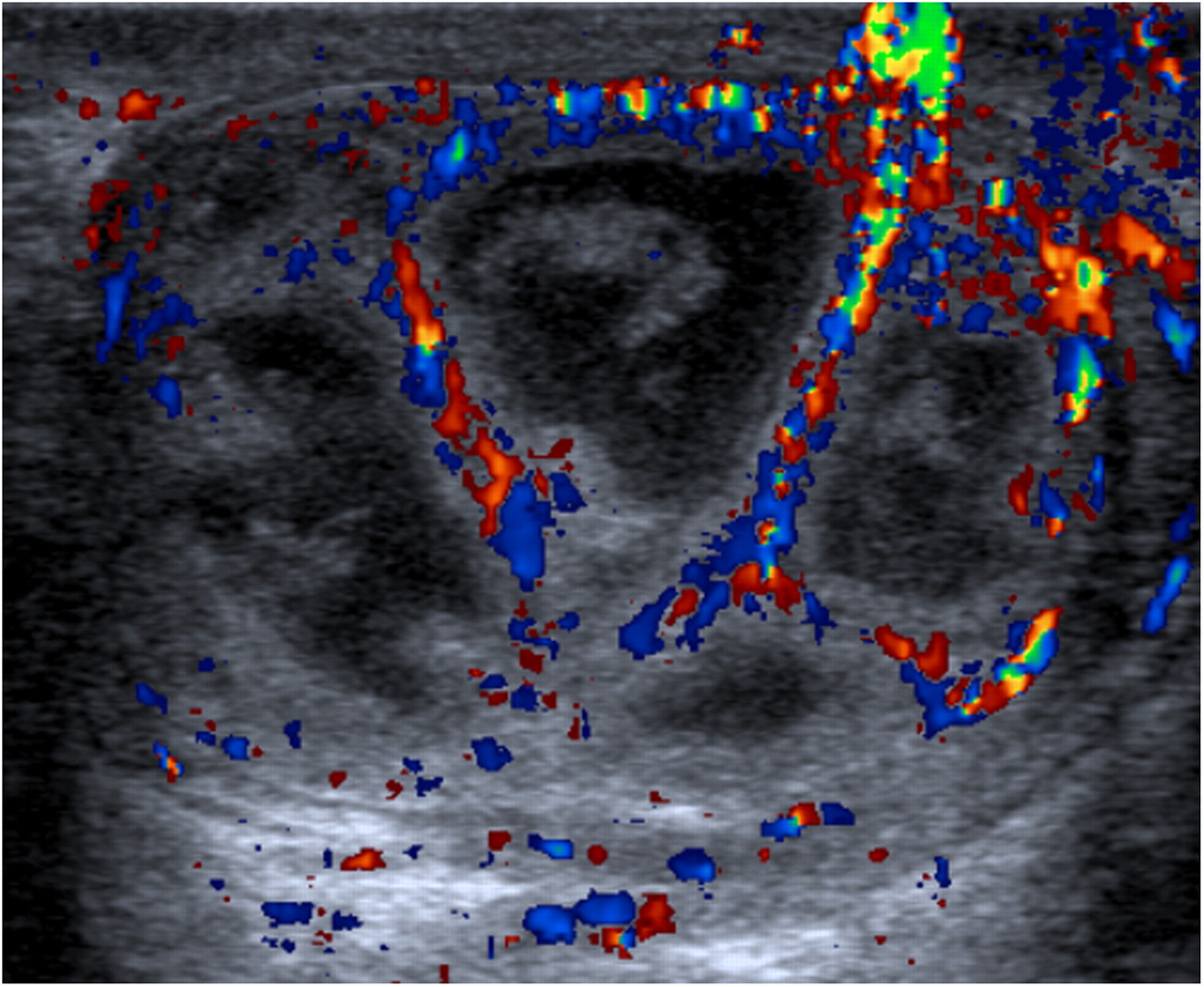
Doppler ultrasound of the right testis showing the increased peripheral vascularity surrounding segmented cystic areas
Following ciprofloxacin, his right testis appeared of normal size and was no longer painful. Repeat USS showed persisting necrotic areas (Figure 2). A decision to perform a right-inguinal radical orchidectomy was made in consultation with the patient due to concerns of malignancy.

Follow-up ultrasound scan of right testis showing persisting necrotic areas
Macroscopic histology revealed a 4.5 cm × 3.5 cm × 2.2 cm right testis and a 20 mm-wide normal spermatic cord. Sections of the testes revealed a well-circumscribed lesion, yellow in colour with focal areas of necrosis. Microscopically, the lesion was inflammatory granulation tissue, with central necrosis and abscess formation (Figure 3). The granulation tissue contained plasma cells; however, there were no granulomas to suggest tuberculosis (Figure 3). Around the periphery of the lesion there were thickened vessels and endarteritis. Stains for acid-fast bacilli and fungi were negative. There was no evidence of malignancy. Serological studies for tuberculosis and lymphogranuloma venereum (Chlamydia trachomatis) were negative.
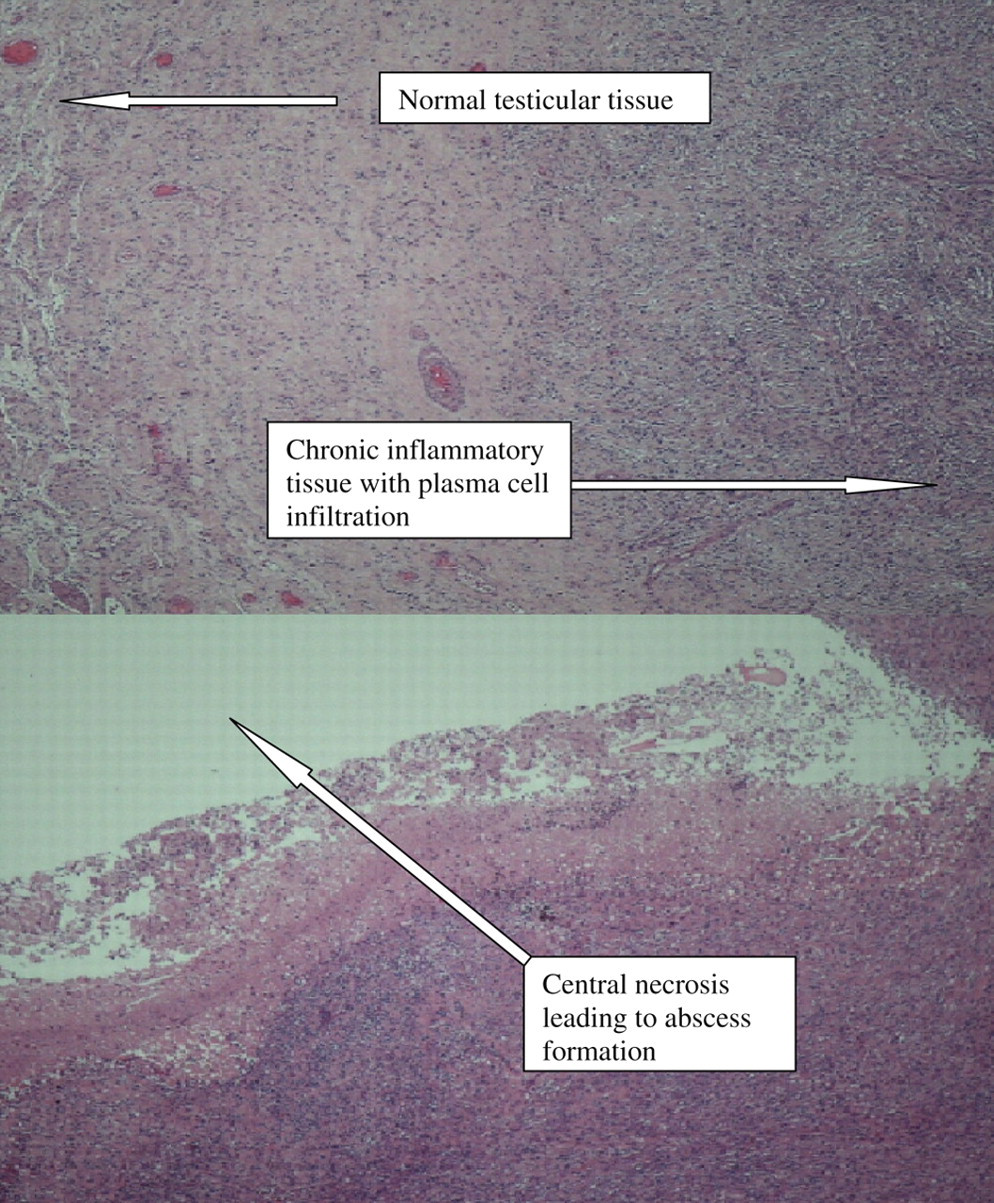
Histology slides of the right testis post-orchidectomy revealing chronic inflammatory tissue with plasma cell infiltration and central abscess formation
However, syphilis serology was positive. The Venereal Disease Research Laboratory (VDRL) test was negative, but the Trepenoma pallidum particle agglutination (TPPA) and fluorescent treponemal antibody absorption (FTA-Abs) tests were both positive. He was diagnosed with syphilitic orchitis and treated with three intramuscular injections of 2.4 MU of benzathine penicillin at weekly intervals. At six-month follow-up, he was well with no clinical or serological evidence of recurrence and the VDRL remained negative.
DISCUSSION
Syphilis, first described in 15th-century Europe was endemic by the 17th century. 1 Since 1996, syphilis incidence has more than doubled in the UK, driven by localized outbreaks, (London 2001) secondary to the HIV epidemic and high-risk groups, e.g. men who have sex with men. 2
The sexually transmitted spirochete, Treponema pallidum subsp. pallidum, is highly invasive. 3 One month after infection, the primary painless chancre appears with localized lymphadenopathy. 4 During this period there is dissemination throughout the body. Secondary syphilis occurs typically within two to three months of infection, and may present with a maculo-papular rash, generalized lymphadenopathy, condylomata lata, fever, aches and malaise. 5 Symptoms resolve spontaneously after a few months as the organism enters a latent phase. 5
Tertiary syphilis occurs 10–25 years after initial infection, coinciding with waning cell-mediated immunity. 4 There are two basic tissue reactions: gummatous necrosis and small vessel inflammation. 4 Gummas are regions of granulomatous tissue and have a tendency for central necrosis. 4 They can occur in any organ, including testes, causing insidious, painless swelling, which can be mistaken for malignancy. 6
Our case presented with epididymo-orchitis, probably due to the testicular lesions providing a nidus for coliform super-infection. The USS raised malignancy concerns despite normal tumour markers. Histology revealed no evidence of malignancy, but was consistent with tertiary syphilis, with granulomatous areas containing central necrosis and surrounding small vessel inflammation.
Given his unremarkable personal and sexual history it was not until this point that syphilis was considered. Serology confirmed syphilis exposure; the negative VDRL suggested latent syphilis (less common in the presence of the active lesion). This is possibly due to the course of erythromycin received prior to testing. Although erythromycin is not routinely used, it has been shown to have some efficacy against T. pallidum. 3,7
FTA-Abs and TPPA tests usually remain positive for life and do not correlate with disease activity; therefore, follow-up relies on negative VDRL at six and 12 months to confirm disease eradication. 3 In this case, VDRL and clinical assessment for evidence of recurrence remained negative.
This case is unusual as the patient seemed low risk for syphilis. Possible explanations include: unwillingness to disclose other sexual contacts, he had forgotten the initial infection due to the latency period or he had contracted it from his wife, who was untraceable.
Following the decline of syphilis in developed countries, syphilitic orchitis is rare. In the last 59 years, only 11 cases of acquired syphilitic orchitis have been reported: three in Japan, six in France and two in the UK. The Japanese cases describe testicular masses caused by tertiary syphilis mistaken for malignancy that required inguinal orchidectomy. 8–10 Varma et al. 11 report the latest case, a 30-year-old HIV-positive Zimbabwean man with acute syphilitic orchitis. Our case was low risk and syphilis was not considered until after histological examination.
The UK syphilis epidemic continues to be predominantly limited to high-risk groups. Future spread into a wider population remains possible but unpredictable. 11 This case illustrates that syphilitic orchitis must be considered as a differential diagnosis if symptoms or radiological signs are atypical or do not resolve after standard therapy. 12