
Abstract
An audit of 72 patients presenting for post-exposure prophylaxis following sexual exposure (PEPSE) to HIV (68 genitourinary medicine and 4 accident & emergency) was conducted from 2003 to 2009. The principal indications for PEPSE included 27 (38%) unprotected intercourse (15/27 vaginal and 12/27 anal) with a known HIV-positive partner, 20 (28%) unprotected receptive anal sex with male partner of unknown status, 17 (24%) following sexual assault and three (4%) unprotected sex with a partner from an endemic country. Of those who commenced PEPSE, 92% did so within the recommended 72 hours. Concurrent sexually transmitted infection (STI) was diagnosed in 8.3% patients (6.9% non-gonococcal urethritis and 1.4% rectal chlamydia). Fifty (69%) patients attended for follow-up and only 8% of these did not complete treatment. Twenty-five (35%) patients attended for repeat serology at three months and 18 (25%) at six months. All of the patients followed up remained HIV-negative.
Keywords
INTRODUCTION
Post-exposure prophylaxis following sexual exposure (PEPSE) is widely accepted as a strategy to reduce HIV acquisition. There have been no randomized clinical trials to prove its efficacy, although prospective data are available comparing outcomes in those who received PEPSE within 72 hours of sexual exposure and those who were not eligible for treatment. 1,2 Fewer seroconversions occurred with PEPSE use. Post-exposure prophylaxis for HIV has been used for many years following occupational exposures 3 and is also given to neonates to reduce vertical transmission. 4,5 Animal studies suggest potential benefit when given following sexual exposure; however, this is dependent on time of initiation and duration of treatment. 6,7 The British Association of Sexual Health and HIV (BASHH) drew up national guidelines in 2006 to provide recommendations on when to consider prescribing PEPSE, appropriate monitoring and follow-up. 8 The aim of this study was to assess the seven-year experience of PEPSE in a regional centre.
METHODS
A retrospective audit was carried out of all patients who received PEPSE from genitourinary (GU) medicine and accident & emergency (A&E) departments from January 2003 to August 2009 inclusive at Royal Victoria Hospital, Belfast, UK. Patients were identified from clinic documentation and pharmacy records. It was not possible to include those patients who were offered PEPSE and declined. Details collected included demographics, indications for PEPSE, time of initiation, adherence and follow-up. The findings were compared with standards outlined in the BASHH guidelines for the use of PEPSE for HIV (2006), although these were not available for the early period of the study.
RESULTS
In total, 72 individuals received PEPSE during the study period (10 of these were managed prior to publication of BASHH guidelines in 2006); 42/72 (58%) of prescriptions for PEPSE were issued within the last two years (Figure 1). The majority of patients (51%) were men who have sex with men (MSM), with heterosexual men and women accounting for 18% and 31%, respectively. Time from sexual exposure to initiation of PEPSE was less than 72 hours in 92% (target 90%), with 28% of patients receiving treatment within 12 hours. A recommended regimen was used in 69 (96%) patients and this reflected the antiretroviral agents available at that time; 93% of prescriptions were given for an exposure in accordance with recommendations (target 90%). This included 20 (28%) patients who had unprotected receptive anal intercourse with casual partners of unknown status, three (4%) unprotected contact with partners from an endemic country and 17 (24%) following sexual assault. Of the sexual assault cases, five (29%) were male assaults and a further five (29%) involved assailants from a country of high HIV prevalence. Twenty-seven (38%) patients were sexual contacts of HIV-positive individuals; of these, 3/27 (11%) were partners of newly diagnosed patients, and 19/27 (70%) of these HIV-positive individuals were known to our HIV clinic. Six of them (32%) were well established on antiretroviral therapy with an undetectable viral load at last check and none had drug resistance that precluded the use of standard antiretroviral agents for PEPSE. Of the source patients, one was hepatitis C RNA positive and another was a chronic carrier of hepatitis B (hepatitis B e-antigen negative). Forty-nine (68%) patients accepted a screen for sexually transmitted infections (STIs). The rate of concomitant STIs among those tested was 14%, with six (12%) patients being treated for non-gonococcal urethritis and one (2%) for rectal chlamydia. Twenty-two (31%) of patients did not attend for follow-up after commencing treatment, including all four patients who received PEPSE from A&E. Of the 50 patients who attended for review, only four (8%) did not complete treatment. All four were due to re-evaluation of their risk and not as a result of poor tolerability. This compares favourably with the target outcome for completion of 75%. No serious adverse events were reported; however, minor side-effects were noted in 62% (31/50) patients. Of those 31 patients reporting side-effects, 20 (65%) received a regimen containing a nucleoside backbone of zidovudine and lamivudine versus 11 (35%) whose regimen contained tenofovir and emtricitabine. Reported side-effects included diarrhoea (36%), nausea (32%) and headache (5%). Twenty-five (35%) patients attended for repeat serology at three months and only 18 (25%) attended at six months, which was considerably below the BASHH-recommended target of 60%. All tested negative for HIV, syphilis and hepatitis B and C. A further eight patients tested negative for HIV at subsequent GU medicine attendances.
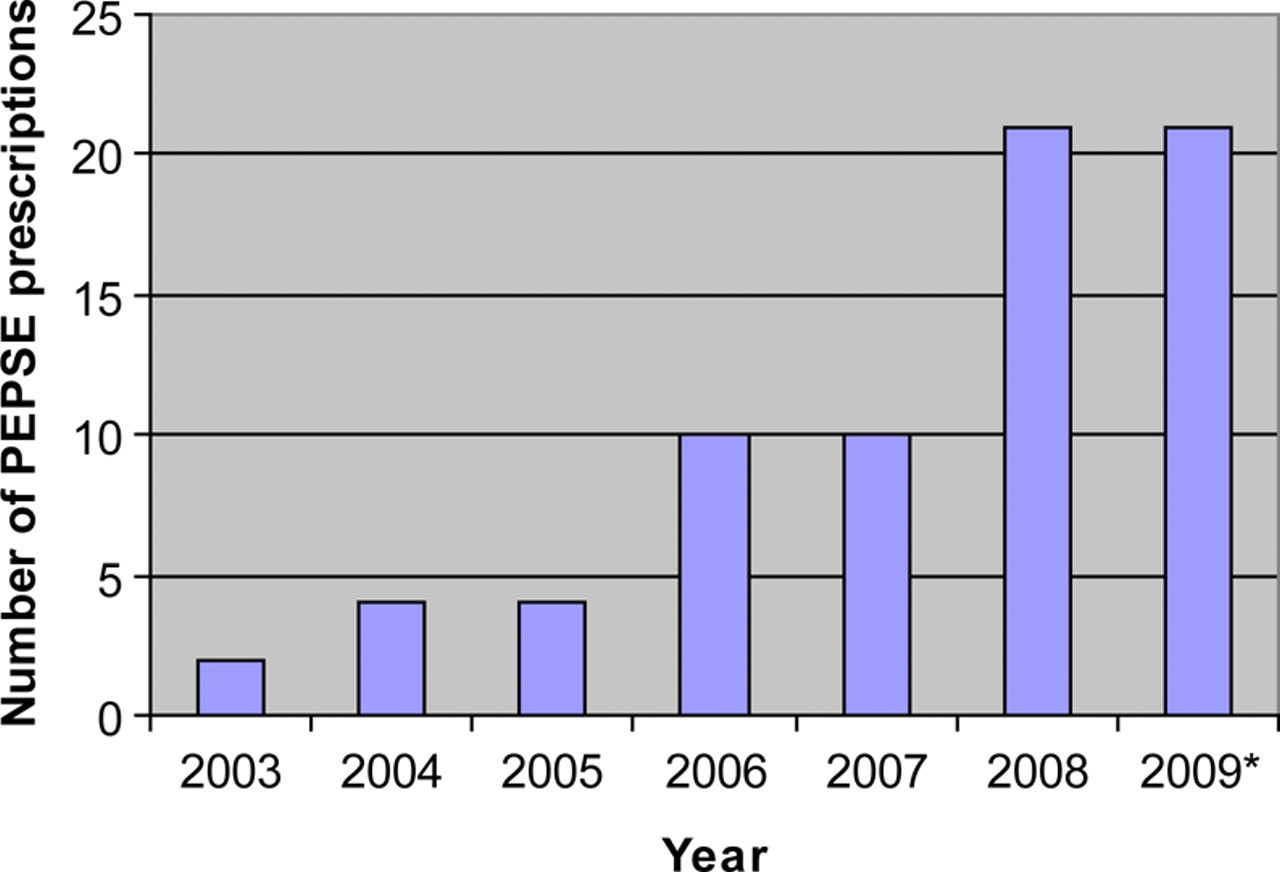
Trend in PEPSE prescribing over seven years. *Data only collected until August 2009 inclusive
DISCUSSION
There has been a dramatic increase in the use of PEPSE over the last few years. This is likely to be as a result of increased awareness among high-risk groups and improved access to GU medicine services. It is also reflective of the level of ongoing high-risk sexual behaviour, especially among MSM. Concerns have been expressed that providing PEPSE may actually promote unsafe sexual practice 9 ; however, evidence of this is lacking. 10–12 Furthermore, offering PEPSE creates an opportunity to test for other STIs and facilitates discussion regarding risk reduction and safer sex. All patients commenced on PEPSE at our clinic are offered a full STI screen and the high rate of concomitant infection was as expected. The absence of any cases of infectious syphilis or gonorrhoea was however surprising. Hamlyn et al. 13 reported similar concurrent infection rates among 253 patients receiving PEPSE, with 4.5% and 2.5% being treated for chlamydia and gonorrhoea, respectively.
It is reassuring, but not unexpected, that no seroconversion took place among our patients. Side-effects tended to occur more frequently with the earlier antiretroviral agents, e.g. zidovudine compared with the regimen of tenofovir, emtricitabine and ritonavir-boosted lopinavir that is offered at present. 14
This audit highlights a need to improve links between departments providing PEPSE, as those patients from A&E did not attend GU medicine for sexual health testing or advice. A protocol for risk assessment and prescribing of PEPSE is under development for use in A&E departments in Northern Ireland, which will include a GU medicine referral pathway. Methods of improvement for ease of review included specific allocation of appointment, telephone and text message reminders and health adviser follow-up. Current recommendations are for repeat HIV testing at three and six months after PEPSE; however, with newer fourth-generation HIV antibody/antigen assays it may be possible to revise this. A re-audit has been planned for 2013.