
Abstract
This study evaluated a population with a relatively low prevalence of gonococcal (GC) infection attending a genitourinary (GU) medicine clinic. Nucleic acid amplification testing (NAAT) screening was compared with culture. A total of 2004 male urine, 1699 female endocervical and 424 self-taken vulvovaginal swabs were screened using the BD ProbeTec GC NAAT alongside Neisserial culture. ProbeTec-positive samples confirmed by the Gen-Probe Aptima GC NAAT and/or culture positive were deemed to have GC infection. Thirty-three out of 4157 (0.8%) specimens gave a reactive result by BD ProbeTec NAAT. Twenty-two were confirmed by Gen-Probe Aptima NAAT alone (4), culture alone (7) or both (11). Four patients were identified with GC infection who would have been missed by standard culture. No samples were culture positive and ProbeTec NAAT negative. Of 11 unconfirmed reactive samples, five gave low readings and three were contacts of gonorrhoea. Screening for Neisseria gonorrhoeae using NAAT is a viable alternative to culture even in a low-prevalence population.
Keywords
BACKGROUND
In the UK, there has been a decline in gonococcal (GC) infections in recent years, although levels still remain relatively high among young people. 1,2
The national picture has been mirrored within Torbay (a seaside resort) where an audit of genitourinary (GU) medicine services in 2003 showed an overall incidence for GC of 1.3% among clinic attendees, which had fallen to 0.5% by 2007. However, detecting GC in genital samples traditionally relies on routine culture, which involves taking endocervical or urethral samples. Endocervical sampling can be uncomfortable for women, who may decline to be tested; similarly, urethral sampling can be painful for men. Young people, in particular, are often reluctant to undertake invasive sampling, particularly in the absence of symptoms. 3
As part of a national strategy to reduce Chlamydia trachomatis (CT) infections, the Department of Health introduced a national chlamydia screening campaign using local laboratories, which introduced nucleic acid amplification tests (NAAT) for sexually active people aged 16–24 years in England. 4 One major advantage with this development is that non-invasive NAAT can now be offered to all sexually active people through GU medicine clinics, family planning clinics and general practice (GP) surgeries. 5 Many manufacturers that provide NAATs for CT are also able to provide a NAATs for GC performed simultaneously on the same sample.
Concerns, however, have been expressed about the predicted high number of false-positive results that may occur with GC NAAT screening, particularly in a low-prevalence population, and the impact this could have on both the patient and sexual health services. 6 In light of this, a decision was made within Torbay to undertake combined NAAT testing for CT and GC in a GU medicine clinic with a relatively low incidence of GC, and compare this with conventional culture for GC. If found to be useful, such non-invasive tests could be rolled out further to GP practices and family planning clinics to encourage better uptake of opportunistic STI screening among the at-risk, sexually active population.
METHODS
Over a one-year period (April 2008–March 2009), patients were tested for evidence of Neisseria gonorrhoeae and CT infection using the BD ProbeTec GC/CT NAAT assay (Becton-Dickinson Diagnostic Systems, Sparks, MD, USA) in addition to routine microscopy and culture for N. gonorrhoeae.
The tests were undertaken at the GU medicine clinic in line with regional and national testing guidelines. 3,7 For symptomatic men, a urine for GC/CT NAAT plus a urethral swab for GC culture was taken. For symptomatic women, endocervical specimens for GC/CT NAAT plus an endocervical and urethral swab for GC culture were taken.
For asymptomatic men, a first-pass urine sample was taken and for women, an endocervical swab was taken. Asymptomatic women who were unwilling to undergo a speculum examination were offered self-taken vulvovaginal swabs for combined GC/CT NAAT. Non-genital specimens (e.g. rectal and throat swabs) when taken, were submitted for GC culture alone.
Information was provided to patients in the GU medicine clinic about the nature of the screening test and they were advised that if GC infection could not be excluded on the initial samples, then further follow-up, including additional investigations, would be offered.
All non-culture specimens were initially processed with the BD ProbeTec platform and samples giving a GC-reactive result were sent to the Bristol Regional Health Protection Agency (HPA) laboratory for confirmatory testing using the Aptima GC (Gen-Probe Inc, San Diego, CA, USA) NAAT. Based on the manufacturer's instructions, a ProbeTec GC-reactive result was defined as having a method other than acceleration (MOTA) score of greater than 2000. The MOTA score is a metric method used to assess the magnitude of signal generated as a result of the reaction. Any readings between 2000 and 10,000 were classified as provisional low positives, whereas any readings greater than 10,000 were classified as provisional positive.
Patients with a reactive result were recalled for further testing if no culture specimen had been taken. The criteria for determining a confirmed GC-positive result was based on the finding of either a positive culture alone or a reactive ProbeTec GC NAAT with either a positive GC culture or a positive Aptima GC NAAT or a combination of positive GC culture and positive Aptima GC NAAT.
Patients confirmed by Aptima NAAT and/or GC culture were re-assessed for further testing, treatment, follow-up and partner tracing as necessary.
Patients with inhibitory results for GC NAAT had their initial specimen retested. If these remained inhibitory then further specimens, including swabs for culture, were requested.
RESULTS
In all, 1699 endocervical, 33 urethral, 424 self-taken vulvovaginal swabs and 2004 first-pass urine samples were evaluated on the ProbeTec-combined GC-CT NAAT platform. Of the 4160 specimens tested (for GC and CT), 33 (0.8%) were determined as initially reactive by ProbeTec GC NAAT. Figure 1 shows the break down of reactive specimens based on specimen type.
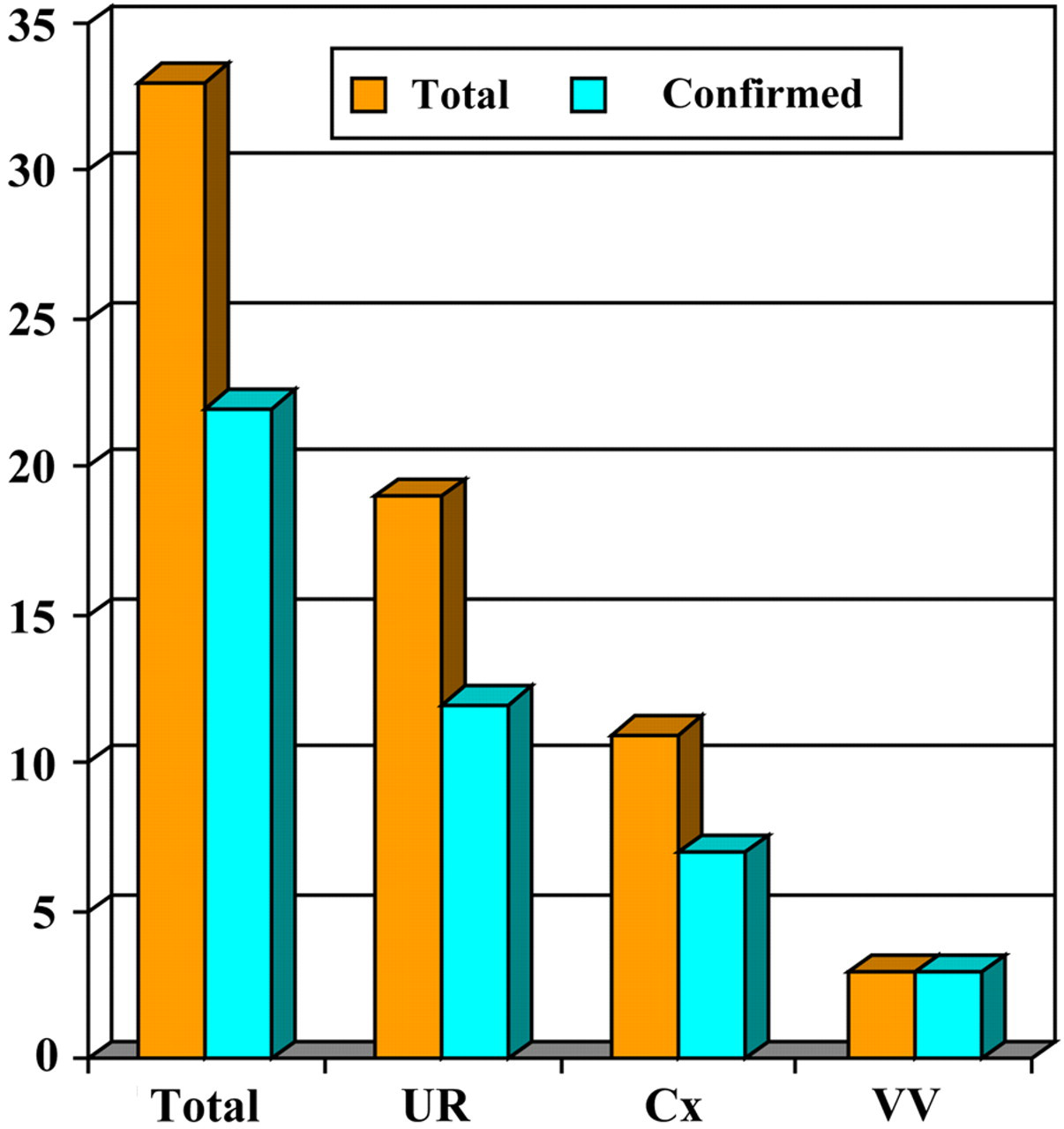
Distribution of BD ProbeTec-reactive gonococcal samples (total and confirmed) by specimen type. UR, urine; Cx, cervical swab; VV, vulvovaginal swab
Twenty-two (0.5%) of the reactive specimens were confirmed by either Aptima GC NAAT (4), positive GC culture (7) or both (11). Three of the GC-culture-positive patients also had an equivocal Aptima GC NAAT result.
Of the four patients confirmed by Aptima GC NAAT alone, three were negative on culture and the other patient had declined urethral culture. This patient named a pregnant woman as a contact, who subsequently tested positive for CT and was reactive for GC on ProbeTec, but remained unconfirmed by both Aptima and GC culture.
Of the 11 reactive specimens that were unconfirmed, five gave low-level positive NAAT results (MOTA score > 2000 but <10,000). No samples with a low-level positive MOTA score were confirmed as positive by culture and/or confirmatory test. Of the six remaining unconfirmed reactive samples with an MOTA score >10,000, two were known contacts of patients with gonorrhoea and two failed to return for confirmation.
Overall, 1.1% of specimens gave inhibitory results and were re-tested. None of these patients had positive cultures for GC.
Of all the cultures submitted, no culture-positives would have been missed if NAAT screening alone had been used as a sole screening test. In addition, based on first-pass urines for men and self-taken vulvovaginal swabs for women, over half the cohort were spared potentially uncomfortable and invasive sample collections.
In terms of follow-up, eight patients were recalled. Five required one phone contact, one required three phone contacts and another required five phone contacts. The remaining individual failed to respond to 12 phone contacts, two letters and a home visit. Of the seven patients who responded to tracing, four were confirmed on repeat testing by culture to have had gonorrhoea. No additional contact tracing was required as a result of the delay in diagnosis.
CONCLUSION
The widespread introduction of dual NAATs within local diagnostic laboratories has facilitated combined GC and CT testing. 5,8,9 Concerns have been raised regarding the use of such an approach as high numbers of false-reactive GC results may arise in a low-prevalence population. An additional concern is that relying on NAAT testing/confirmation will result in a lower number of culture isolates available for monitoring antimicrobial resistance trends. GC NAAT-reactive results need to be interpreted with caution and should not be regarded as positive until confirmatory information is available. Some countries, including Scotland, have developed an algorithm for confirmatory testing by specialist laboratories. 10 Advantages of the latter approach are that (in combination with an independent confirmatory NAAT) expertise is readily available for interpretation of results.
Other advantages of using a combined NAAT screening approach for CT and GC infection in a low-prevalence population include the use of the same sample for two different STI tests, reduced laboratory time in processing investigations, decreased turn around time for GC-negative results (98.1% of samples in Torbay) and improved patient acceptability. 8
Problems with routine culture include the requirement for samples to be taken using invasive techniques, the necessity for access to laboratory facilities within a 24-hour period and a significant delay before determining whether a sample is culture negative. Another disadvantage is that culture may be less sensitive than NAAT and so infection could be missed. 3 In this evaluation, cases were identified that would otherwise have been missed if relying on culture alone.
The additional costs of undertaking a GC NAAT test (approximately £3.50 in 2009) is more than offset by laboratory and staff costs if routine culture for asymptomatic patients/non-contacts was to be discontinued. Also, staff time can be saved by patients obtaining their own samples as well as equipment savings (e.g. specula, additional swabs).
Disadvantages of using combined GC/CT NAATs for asymptomatic patients/non-contacts in the absence of routine culture include the need for education and training, difficulty in monitoring GC antibiotic resistance patterns, delays in obtaining confirmation of reactive samples by a second GC NAAT, uncertainty about the use of NAATs on non-genital specimens (e.g. throat or rectal swabs) and the need to recall a small number of patients for further confirmatory testing.
Low-level positive results also need to be interpreted with caution as none of these were confirmed by culture or confirmatory NAAT in our study. In contrast, the use of a higher cut-off based on an MOTA score of >10,000 has been shown to have concordance with positive cultures of 94% in GU medicine attendees in Sheffield. 8
A more recent study has demonstrated that confirmation of ProbeTec GC NAAT samples can be improved further by re-processing the original swab for analysis using a different NAAT platform rather than re-testing the original reaction mix. 11 The number of confirmed ProbeTec GC NAAT-positives rose from 57% to 97% by Aptima NAAT using this modification. This modified method for confirming reactive specimens is now in use in Torbay.
In summary, provided adequate care is taken with interpretation of results, combined NAAT screening for CT and GC is a viable and cost-effective alternative to single CT NAAT screening and conventional GC culture, even in a low-prevalence population, and offers a much more acceptable method for testing in many patients. Careful follow-up with confirmatory testing and/or culture with antimicrobial susceptibilities remains essential for best practice.